Double Board Certified · Specialised Sinus Care
Fungal Sinusitis — a different organism, a different treatment plan.
Fungal sinusitis comprises a spectrum of conditions — from indolent fungus ball to allergic fungal sinusitis to the rare and aggressive invasive forms.…
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"Fungal sinusitis is not one disease. It is several — and the treatment for each is different."
A Note from Dr. Mourad
"Fungal sinusitis comprises a spectrum of conditions — from indolent fungus ball to allergic fungal sinusitis to the rare and aggressive invasive forms. Correct identification of the type drives all subsequent decisions."
— Dr. Moustafa Mourad, MD
Overview
What is fungal sinusitis?
Fungal sinusitis is a group of distinct conditions in which fungal organisms colonize or invade the sinus cavities. Clinically the main forms are: a non-invasive fungal ball (mycetoma), allergic fungal rhinosinusitis (AFRS) driven by an immune response to fungal antigens, and invasive fungal sinusitis, which is rare and serious and occurs primarily in immunocompromised patients.
Symptoms overlap with other chronic sinus disease — obstruction, post-nasal drip, facial pressure, loss of smell — but examination, nasal endoscopy, and CT imaging often show characteristic findings such as unilateral disease, dense calcifications, or expansile mucin.
Treatment depends on the type. Fungal balls are removed surgically. Allergic fungal sinusitis requires surgery plus long-term medical management of the inflammatory disease. Invasive fungal sinusitis is a medical and surgical emergency. Accurate classification is essential to choosing the right pathway.
Key takeaways
- Fungal sinusitis is a spectrum of conditions, not a single disease.
- Non-invasive forms include the fungus ball and allergic fungal rhinosinusitis (AFRS).
- Invasive fungal sinusitis is rare, occurs mainly in immunocompromised patients, and is a surgical emergency.
- Fungal balls are removed surgically; allergic fungal sinusitis adds long-term medical management.
- Accurate classification — urgent versus elective — drives every treatment decision.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
Castle Connolly Top Doctor — Plastic Surgery, 202602 · Symptoms
How this condition typically presents.
Three patterns are most common. Patients often recognise themselves in one or more of these.
I
Chronic Unilateral Symptoms
One-sided congestion, drainage, or facial pressure that does not respond to standard treatment — a pattern suggestive of fungal disease.
II
Nasal Polyps with Thick Allergic Mucin
Patients with extensive polyps and thick, eosinophil-rich mucin — characteristic of allergic fungal sinusitis.
III
Rapid Progression in Immunocompromised Patients
Fever, facial pain, visual changes, or neurologic symptoms in an immunocompromised patient — a possible presentation of invasive fungal sinusitis and a surgical emergency.
03 · Anatomy
Non-invasive vs invasive fungal sinusitis.
The single most important distinction — non-invasive disease is treated electively, invasive disease is a surgical emergency.
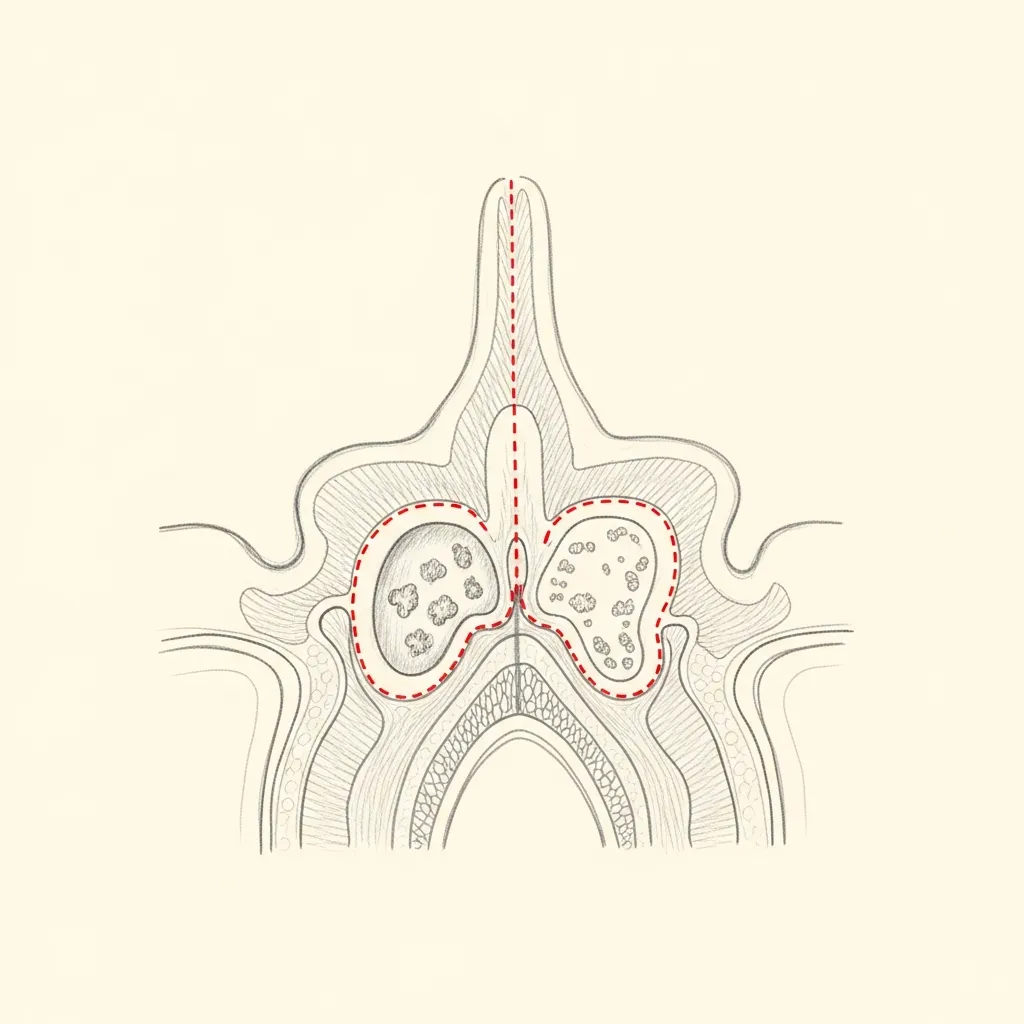
Non-Invasive
Fungal ball & allergic fungal sinusitis
A fungal ball is a discrete collection of fungal hyphae within a sinus — usually in immunocompetent patients, treated definitively with endoscopic clearance.
Allergic fungal sinusitis presents with polyps and characteristic allergic mucin; treatment combines surgical clearance with ongoing medical therapy to control the inflammatory response.
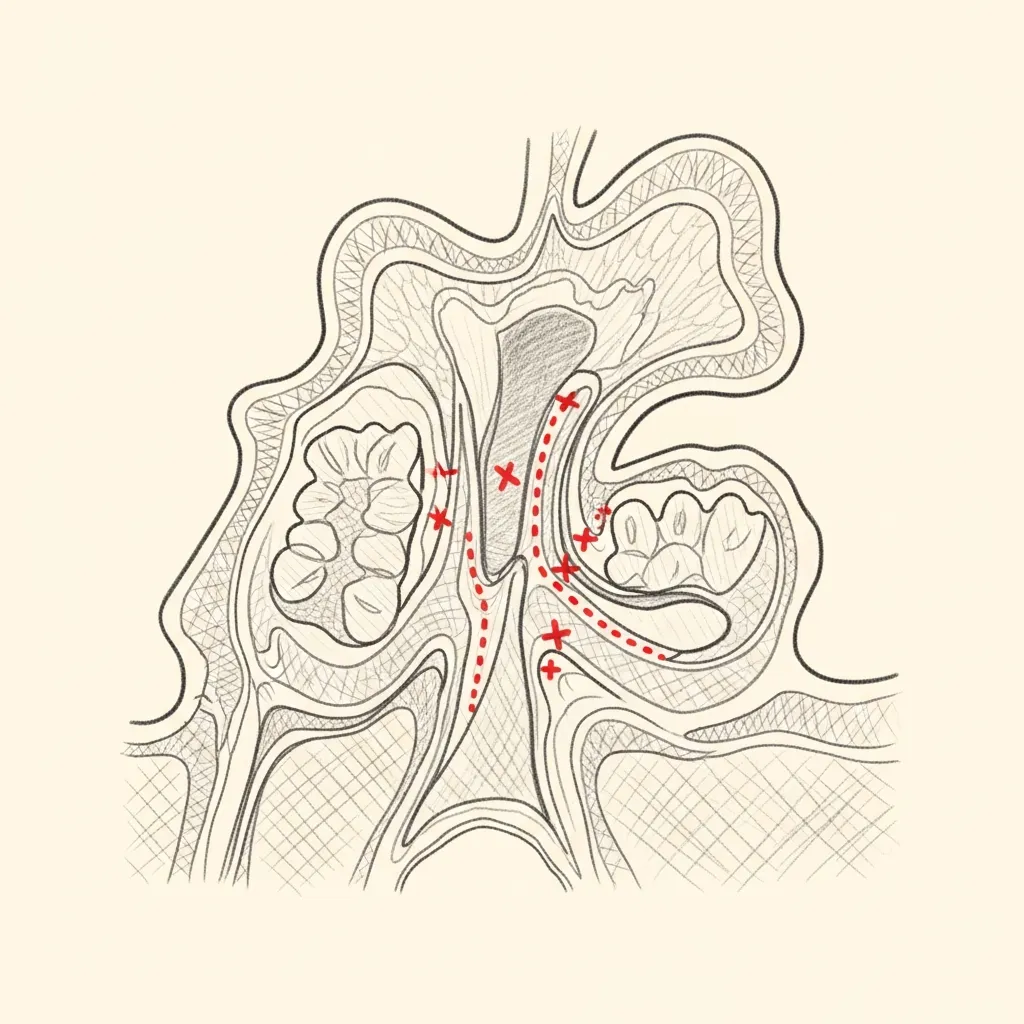
Invasive
A surgical emergency
Invasive fungal sinusitis is uncommon but life-threatening, occurring most often in patients with diabetes, immunosuppression, or hematologic malignancy.
Management is urgent and combined — aggressive surgical debridement, systemic antifungal therapy, and coordination with infectious disease and the patient's primary specialist.
Illustrative diagrams. Suspected invasive fungal sinusitis is evaluated urgently.
04 · Diagnosis
How the diagnosis is made.
Diagnosis begins with endoscopy and CT imaging — characteristic findings often distinguish fungal disease from bacterial.
Intra-operative pathology and microbiology confirm the type.
In suspected invasive disease, urgent imaging and biopsy take priority over any other workup.
05 · Treatment Options
Treatments matched to the diagnosis.
Treatment is individual. The right answer ranges from optimised medical therapy to a focused procedure to definitive surgery.
Endoscopic Sinus Surgery
Surgical clearance is the cornerstone of treatment for non-invasive fungal disease.
Learn More
Adjunctive Medical Therapy
Topical steroids, immunomodulation, and selective antifungal therapy for allergic fungal sinusitis.
Learn More
Aggressive Management of Invasive Disease
Coordinated surgical and systemic antifungal management for invasive fungal sinusitis.
Learn More
01 · Why Dr. Mourad
Diagnosis first, treatment second.
Dr. Mourad evaluates fungal sinusitis with awareness of the full spectrum — most cases are non-invasive and surgically manageable, but invasive disease is a surgical emergency.
Diagnosis combines endoscopy, CT or MRI imaging, and intra-operative pathology.
Treatment is matched to the type — surgical clearance for fungal ball, surgical clearance plus medical therapy for allergic fungal sinusitis, and aggressive combined management for invasive disease.
When to Seek Care
When to seek care promptly.
Fever, severe facial pain, or visual changes in an immunocompromised patient — evaluate immediately.
Rapidly progressive facial swelling, numbness, or weakness — evaluate immediately.
Black eschar or necrotic tissue in the nasal cavity on examination — surgical emergency.
New neurologic symptoms in a patient with known sinus disease — evaluate immediately.
Outlook
What to expect.
When the diagnosis is correct and the right treatment is applied, the outlook is generally good. Most patients describe meaningful improvement in symptoms and day-to-day function.
When symptoms persist despite treatment, the workup is re-opened. Persistent symptoms with no answer almost always mean the diagnosis is incomplete.

Living Well
Day-to-day measures that help.
Daily saline irrigation, control of indoor allergens, and good sleep hygiene meaningfully reduce day-to-day symptoms for many patients.
Medical therapy, when prescribed, works best when used consistently rather than as needed — this is one of the most common reasons treatment seems to fail.
Frequently Asked
Patient questions, honestly answered.
Distinction begins with history, endoscopy, and CT findings. A unilateral, well‑circumscribed dense sinus opacity with focal bony remodeling favors a fungal ball. Bilateral polyps, tenacious allergic mucin, and atopic history point toward allergic fungal sinusitis (AFS). Definitive confirmation often requires intraoperative inspection and pathology with fungal stains. Final management is decided after in‑person evaluation and tissue review when indicated.
A unilateral dense maxillary opacity increases suspicion for a fungal ball, particularly when CT shows calcifications or localized bony change. Dental disease, prior surgery, and chronic bacterial sinusitis can produce similar appearances. Nasal endoscopy and, when needed, targeted sampling help narrow the diagnosis. Surgical indication depends on symptoms, endoscopic correlation, and shared decision‑making at consultation.
Surgical removal can restore sinus ventilation and sometimes improve smell and congestion, but outcomes vary. Smell recovery is more likely when loss is recent; longstanding anosmia may not fully recover and can take weeks to months if it does. Persistent allergic inflammation or polyps often require additional medical therapy to address residual symptoms. Expectations are individualized and reviewed during the consultation.
Systemic antifungals are generally not recommended for noninvasive fungal balls or routine AFS based on available evidence. Primary treatment for these entities is surgical clearance plus topical therapies such as saline irrigations and topical steroids. Systemic antifungal therapy is reserved for invasive disease or select immunocompromised patients and is prescribed after infectious disease consultation. Medication choices are individualized and balanced against potential side effects and monitoring needs.
Invasive fungal sinusitis can progress over hours to days, especially in patients with uncontrolled diabetes or neutropenia. Early warning signs include rapidly worsening facial pain, fever, periorbital swelling, vision changes, facial numbness, or new cranial neuropathies. Urgent imaging, nasal endoscopy, and biopsy guide immediate management. Suspected invasive disease requires prompt in‑person evaluation and multidisciplinary coordination.
Early postoperative findings commonly include nasal crusting, mild bleeding, and transient congestion. Less common complications are infection, synechiae (scar bands), and the potential need for revision surgery. Rare but serious risks include orbital or skull‑base injury when disease is adjacent to these structures; image guidance and careful technique mitigate risk. Regular postoperative debridement and topical therapy support healing and reduce complication rates.
Allergic inflammation and nasal polyps increase the risk of persistent mucosal disease and recurrence after surgery. Long‑term control typically requires topical steroid therapy, saline irrigations, and collaboration with allergy specialists; immunotherapy is considered when appropriate. Patients with allergic fungal sinusitis often need closer surveillance and intermittent debridement in the first year. Surgery aims to restore drainage so topical treatments can reach the mucosa effectively.
Prior surgery changes anatomy and can create scar that complicates access to fungal disease, especially in lateral recesses or the frontal and sphenoid sinuses. Preoperative CT review, image‑guided navigation, and tailored operative planning are commonly required. Revision cases may need extended endoscopic approaches and closer coordination with infectious disease or allergy colleagues for recurrent disease. Risks, technical complexity, and individualized goals are discussed in detail at consultation.
Continue Reading
Related sinus care
The Most Important Step
Get an expert evaluation.
A careful evaluation by a double board-certified physician is the right first step. The conversation is unhurried, the diagnosis is honest, and treatment is matched to what you actually have.