Double Board Certified · Functional Nasal Care
Chronic Rhinitis — ongoing nasal inflammation has identifiable causes.
Chronic rhinitis is persistent nasal inflammation — allergic, non-allergic, or mixed — that affects daily quality of life. Effective treatment depends on…
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"Most patients with chronic rhinitis have been managing symptoms for years. The first goal is an accurate diagnosis of the type."

A Note from Dr. Mourad
"Chronic rhinitis is persistent nasal inflammation — allergic, non-allergic, or mixed — that affects daily quality of life. Effective treatment depends on identifying the type and matching therapy to the underlying mechanism."
— Dr. Moustafa Mourad, MD
Overview
What is chronic rhinitis?
Chronic rhinitis is persistent inflammation of the nasal lining that produces ongoing symptoms — nasal obstruction, runny nose, post-nasal drip, sneezing, or itching — lasting more than twelve weeks. It is broadly divided into allergic rhinitis, driven by an immune response to inhaled allergens, and non-allergic rhinitis, driven by other triggers such as temperature change, irritants, hormones, or unknown causes.
The condition is common, often under-treated, and frequently mistaken for chronic sinus infection. Distinguishing rhinitis from sinusitis matters because the medical and procedural treatments are different, and antibiotics are rarely the right answer.
Diagnosis combines history, examination, and — when indicated — nasal endoscopy and allergy testing. Treatment is layered: environmental control, intranasal steroids and antihistamines, ipratropium for runny-nose phenotypes, and, in selected refractory cases, in-office procedures targeting the posterior nasal nerve.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — a combination held by a small number of physicians nationally.
02 · Symptoms
How this condition typically presents.
Three patterns are most common. Patients often recognise themselves in one or more of these.
I
Persistent Congestion
Daily nasal obstruction and congestion lasting months or years, often with reduced sense of smell.
II
Runny Nose & Post-Nasal Drip
Clear or coloured nasal discharge and persistent post-nasal drip, often worse on waking.
III
Sneezing & Itching
Recurrent sneezing, nasal itching, and watery eyes — patterns that often point to an allergic component.
03 · Anatomy
Allergic vs non-allergic rhinitis.
The two share symptoms but respond to different treatments. Distinguishing them is the first step toward effective care.
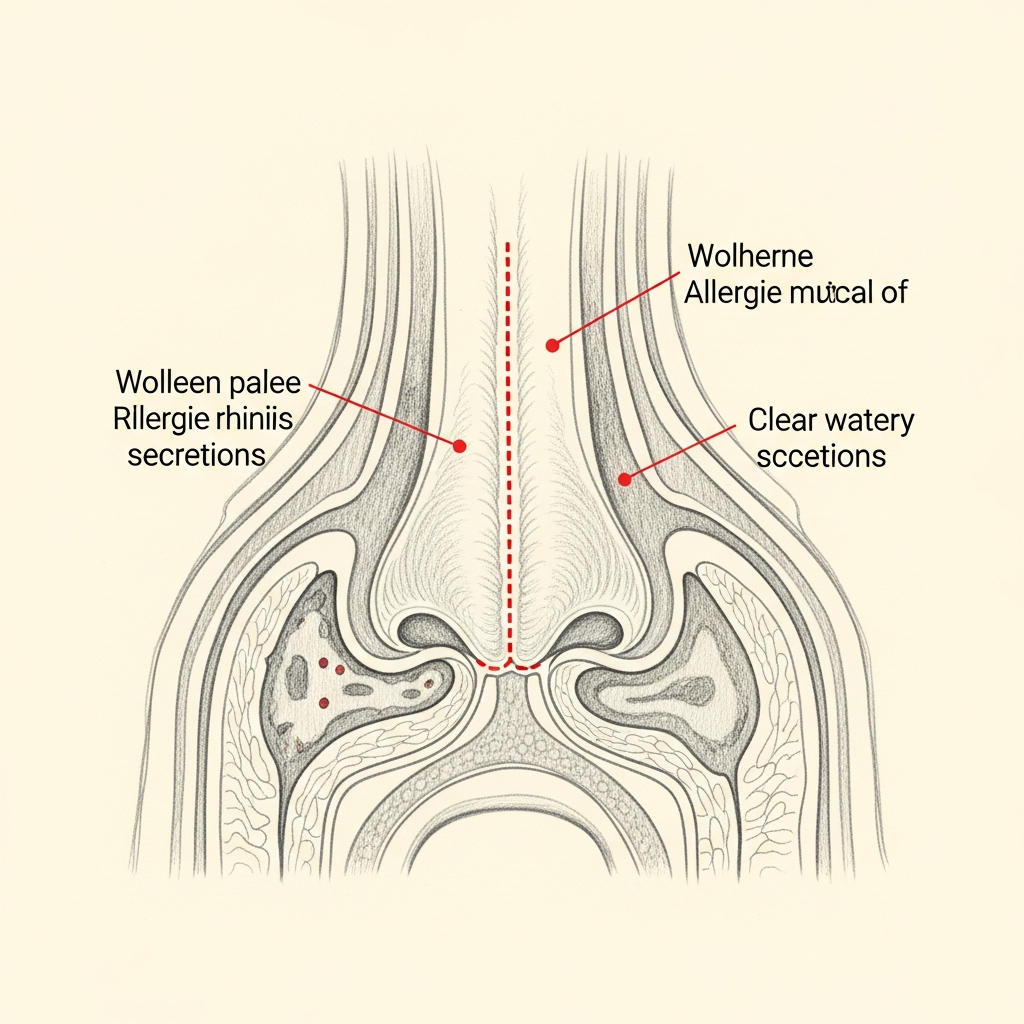
Allergic
IgE-mediated, often seasonal
Allergic rhinitis is driven by IgE-mediated response to specific allergens — often pollen, dust mite, animal dander, or mould. Symptoms are typically seasonal or triggered by exposure.
Treatment includes allergen avoidance, intranasal steroids, antihistamines, and — in selected cases — immunotherapy.
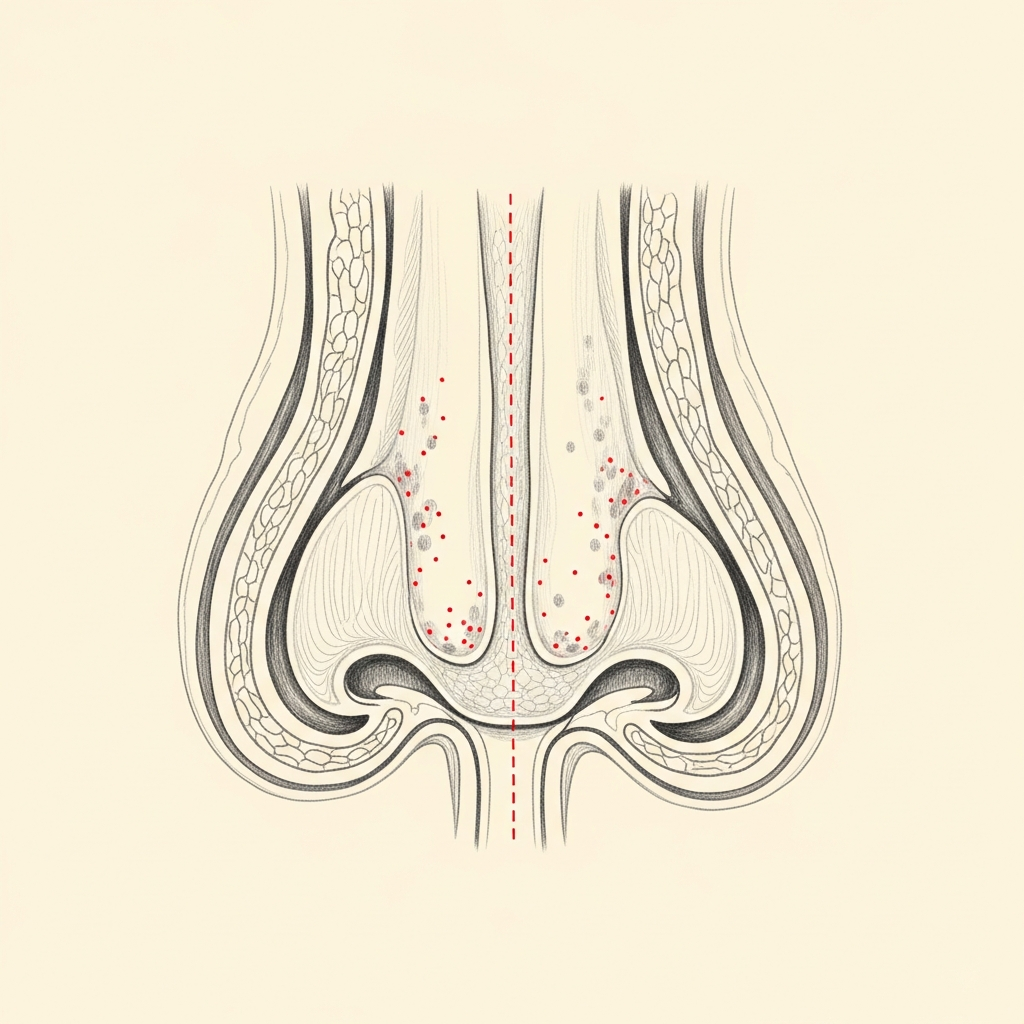
Non-Allergic
Vasomotor or irritant-driven
Non-allergic rhinitis includes vasomotor rhinitis, gustatory rhinitis, drug-induced rhinitis (including rebound from over-use of decongestant sprays), and irritant-driven inflammation.
Treatment is targeted to the specific subtype — and is often very effective once the right diagnosis is made.
Illustrative diagrams. Mixed allergic and non-allergic patterns are common.
04 · Diagnosis
How the diagnosis is made.
Diagnosis begins with a careful history — pattern, triggers, seasonality, and response to prior therapy.
Examination includes anterior rhinoscopy and, where appropriate, nasal endoscopy.
Allergy testing is recommended when the clinical pattern suggests an allergic component.
05 · Treatment Options
Treatments matched to the diagnosis.
Treatment is individual. The right answer ranges from optimised medical therapy to a focused procedure to definitive surgery.
Medical Therapy
Intranasal steroids, antihistamines, saline irrigation, and targeted treatment of allergic triggers.
Learn More
Turbinate Reduction
For patients with persistent obstruction from enlarged turbinates.
Learn More
Vivaer Airway Remodeling
In-office option for selected patients with valve-component obstruction.
Learn More
01 · Why Dr. Mourad
Diagnosis first, treatment second.
Dr. Mourad evaluates chronic rhinitis with a careful diagnostic framework — allergic versus non-allergic, structural versus inflammatory — because the right treatment depends on the right diagnosis.
Medical therapy is optimised before any procedural option is considered.
When procedural treatment is appropriate — for example, posterior nasal nerve ablation for refractory rhinorrhea — it is recommended deliberately.
When to Seek Care
When to seek care promptly.
Severe facial pain, high fever, or visual changes — evaluate urgently.
New unilateral nasal obstruction — evaluate within days, especially in adults.
Bloody nasal discharge that does not resolve — evaluate within days.
Significant facial swelling or redness around the eye — evaluate immediately.
Outlook
What to expect.
When the diagnosis is correct and the right treatment is applied, the outlook is generally good. Most patients describe meaningful improvement in symptoms and day-to-day function.
When symptoms persist despite treatment, the workup is re-opened. Persistent symptoms with no answer almost always mean the diagnosis is incomplete.
Living Well
Day-to-day measures that help.
Daily saline irrigation, control of indoor allergens, and good sleep hygiene meaningfully reduce day-to-day symptoms for many patients.
Medical therapy, when prescribed, works best when used consistently rather than as needed — this is one of the most common reasons treatment seems to fail.
Frequently Asked
Patient questions, honestly answered.
Chronic rhinitis refers to persistent inflammation of the nasal mucosa producing congestion, rhinorrhea, sneezing, or itching. In clinical practice, symptoms present for roughly 12 weeks or more are considered chronic rather than acute. The term describes a pattern, not a single cause, and common contributors include allergic triggers, non‑allergic irritants, medication effects, and anatomic narrowing. Definitive classification requires history, focused examination, and selective testing.
The Most Important Step
Get an expert evaluation.
A careful evaluation by a double board-certified physician is the right first step. The conversation is unhurried, the diagnosis is honest, and treatment is matched to what you actually have.