Double Board Certified · Reconstructive Nasal Care
Septal Perforation — a structural problem with structural and non-structural answers.
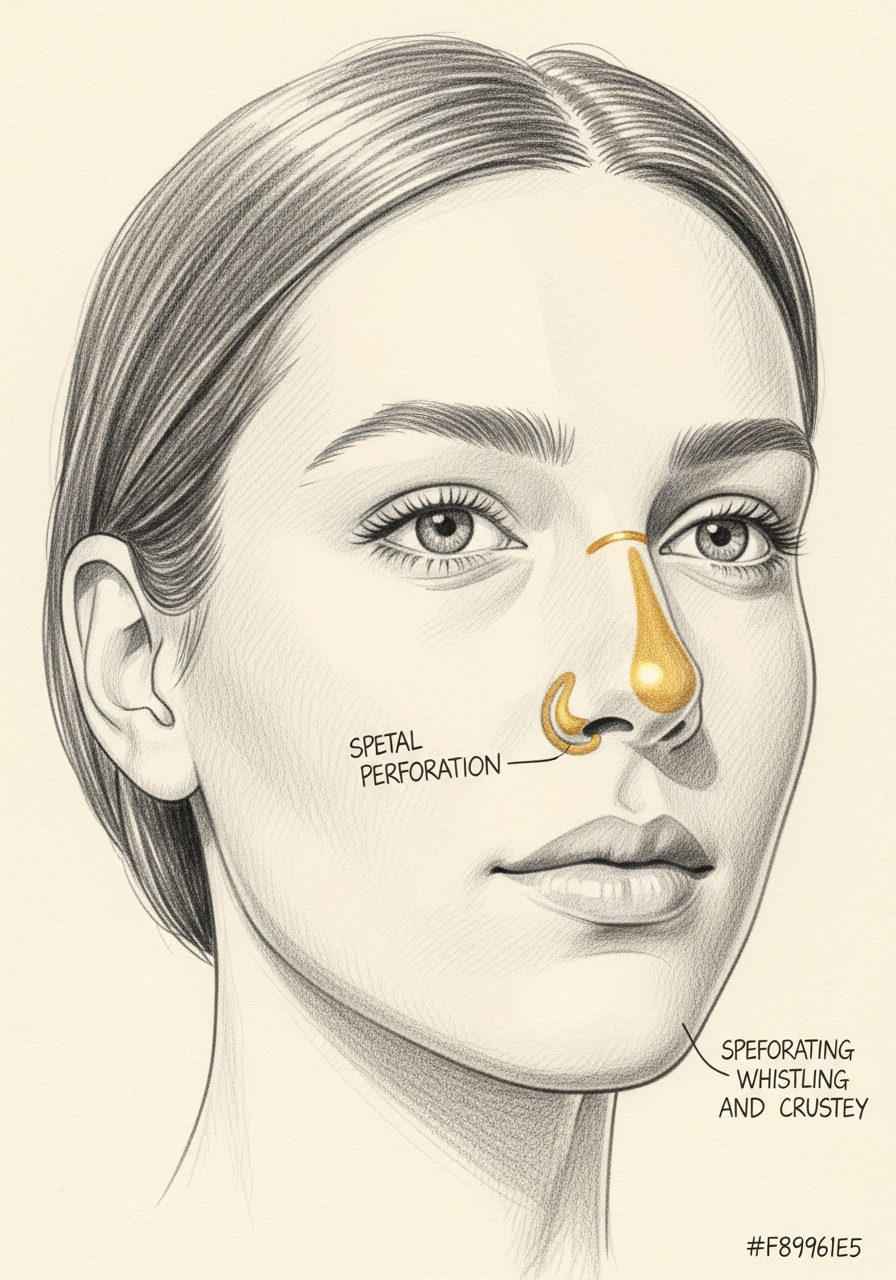
A septal perforation is a hole through the cartilage and mucosa of the nasal septum. The symptoms range from none to severe — whistling, crusting, bleeding,…
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"Not every septal perforation needs to be closed — but every symptomatic perforation needs a careful evaluation by someone who closes them often."

A Note from Dr. Mourad
"A septal perforation is a hole through the cartilage and mucosa of the nasal septum. The symptoms range from none to severe — whistling, crusting, bleeding, and obstruction. Management depends on size, cause, and patient symptoms."
— Dr. Moustafa Mourad, MD
Overview
What is a septal perforation?
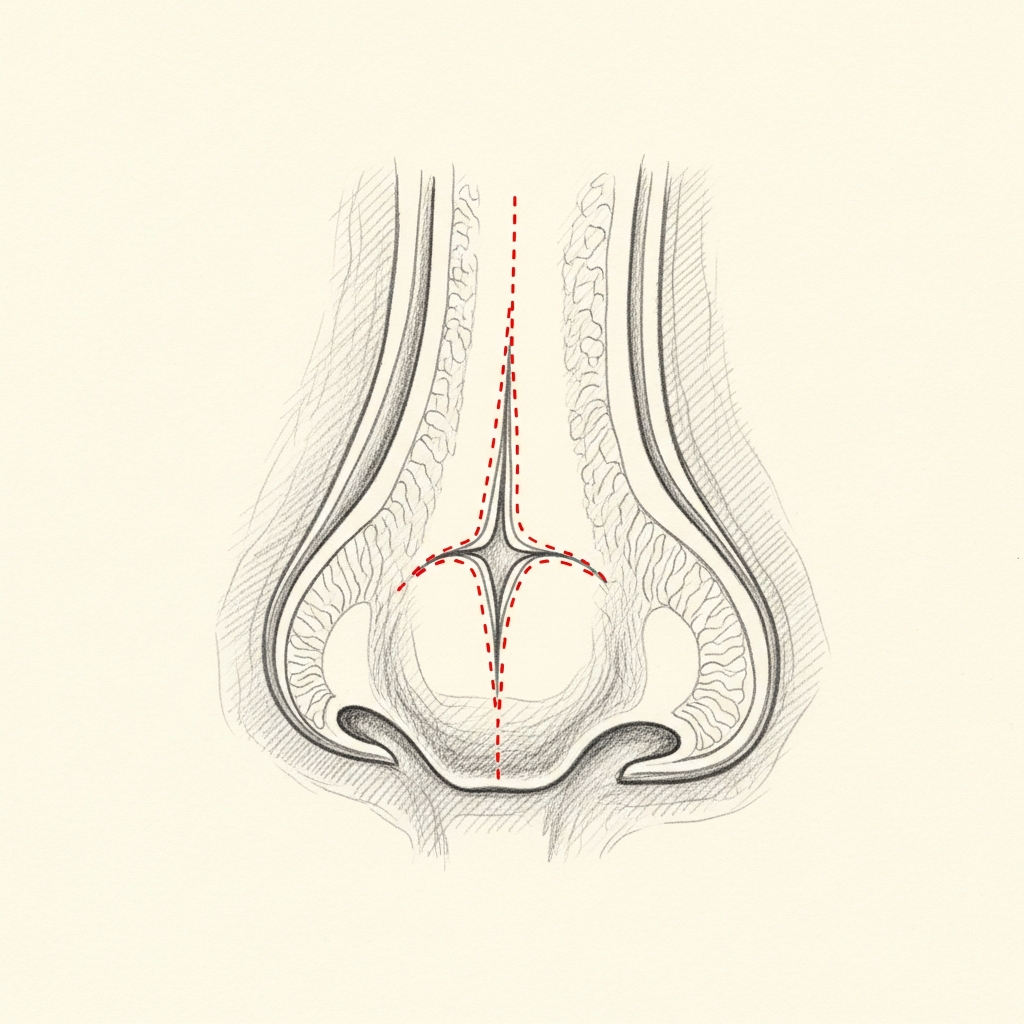
A septal perforation is a hole through the nasal septum — the wall of cartilage and bone that separates the two nasal passages. The perforation spans both mucosal linings and the cartilage between them, creating an abnormal communication between the right and left nasal cavities.
Common causes include prior nasal surgery (especially septoplasty), prior septal cauterization for nosebleeds, intranasal drug use (notably cocaine), chronic intranasal steroid sprays misdirected at the septum, trauma, and granulomatous or autoimmune disease. In some patients no cause is ever identified.
Symptoms depend on size and location: small anterior perforations whistle and crust; larger perforations produce chronic crusting, recurrent nosebleeds, foul smell, and, when very large, dorsal collapse. Asymptomatic perforations are usually managed medically; symptomatic perforations are evaluated for surgical repair.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — a combination held by a small number of physicians nationally.
02 · Symptoms
How this condition typically presents.
Three patterns are most common. Patients often recognise themselves in one or more of these.
I
Whistling & Crusting
A whistling sound with breathing through the nose, and persistent crust formation around the perforation edges.
II
Bleeding & Obstruction
Recurrent nosebleeds, often from the perforation edges, and a sense of obstruction from airflow turbulence.
III
Asymptomatic Perforation
Some perforations cause no symptoms at all — discovered incidentally on examination.
03 · Anatomy
Causes & patterns.
The cause of a perforation shapes the entire management plan. Active inflammatory or drug-induced disease must be controlled before any repair is attempted.
Iatrogenic
Post-surgical perforations
Post-surgical perforations are the most common type seen in revision practice — often discovered weeks or months after septoplasty or rhinoplasty.
These perforations tend to have clean edges and stable surrounding mucosa, making them favourable candidates for surgical closure.
Inflammatory
Active disease must be controlled first
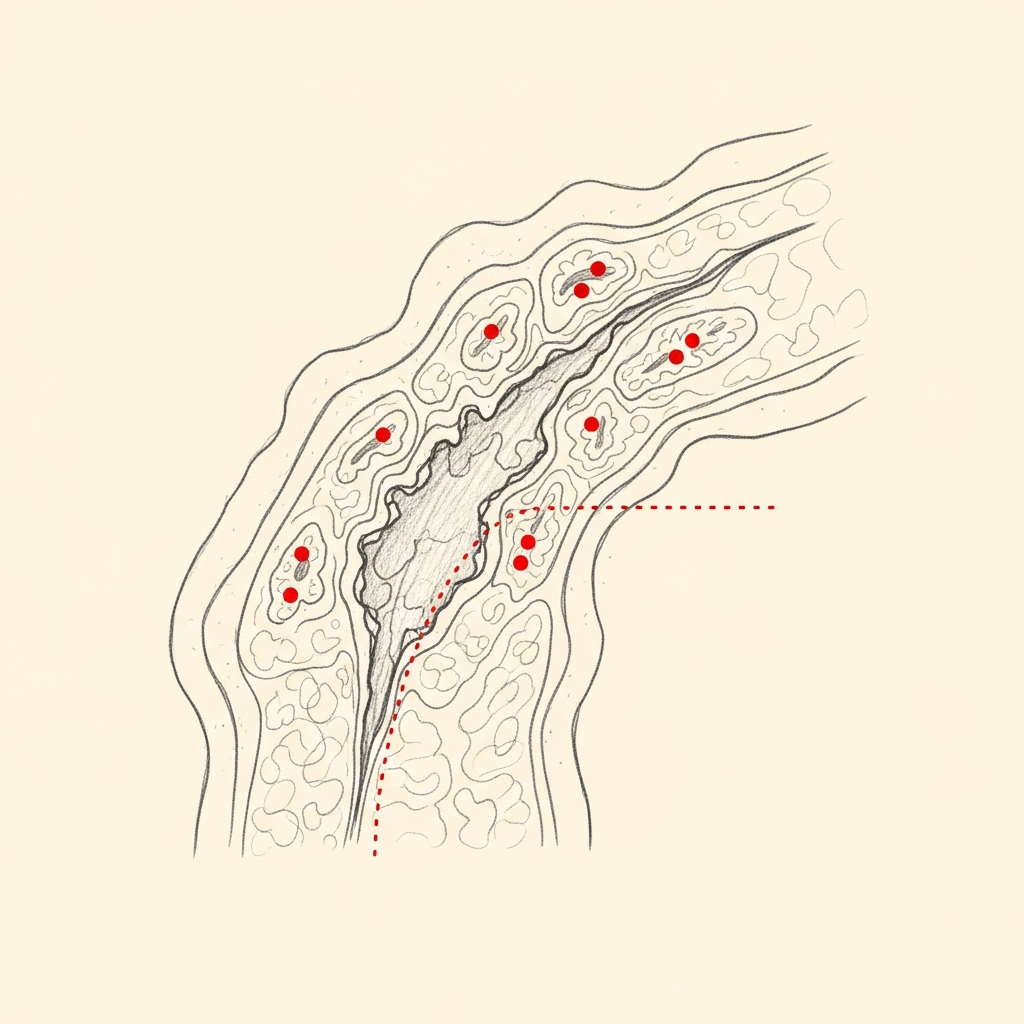
Inflammatory perforations — from granulomatous disease, vasculitis, or intranasal drug exposure — have irregular edges and active surrounding mucosal disease.
Surgical repair will fail unless the underlying disease is controlled. Coordination with rheumatology or appropriate medical specialty is essential before any repair is offered.
Illustrative diagrams. The cause guides everything that follows.
04 · Diagnosis
How the diagnosis is made.
Diagnosis is made on nasal endoscopy — the perforation is directly visible and its size and location documented.
The underlying cause is identified by history and, when warranted, by laboratory workup for inflammatory or autoimmune disease.
CT imaging may be obtained when planning surgical repair.
05 · Treatment Options
Treatments matched to the diagnosis.
Treatment is individual. The right answer ranges from optimised medical therapy to a focused procedure to definitive surgery.
Observation
For asymptomatic perforations — repair is not always indicated simply because a perforation exists.
Learn More
Septal Button
A non-surgical option that closes the perforation mechanically — appropriate in selected cases.
Learn More
Surgical Repair
Definitive closure for symptomatic perforations, with technique matched to size and tissue quality.
Learn More
01 · Why Dr. Mourad
Diagnosis first, treatment second.
Dr. Mourad has a specific practice focus on septal perforation, including cases declined elsewhere.
Evaluation begins with identifying the cause — iatrogenic, traumatic, inflammatory, or drug-induced — because management depends on it.
Repair is recommended when symptoms warrant it and when the underlying cause has been controlled — never reflexively.
When to Seek Care
When to seek care promptly.
Recurrent severe nosebleeds — evaluate within days.
Numbness, weakness, or facial swelling — evaluate immediately.
New rapid enlargement of a known perforation — evaluate within days.
Signs of systemic illness (joint pain, rash, weight loss) with nasal disease — evaluate promptly.
Outlook
What to expect.
When the diagnosis is correct and the right treatment is applied, the outlook is generally good. Most patients describe meaningful improvement in symptoms and day-to-day function.
When symptoms persist despite treatment, the workup is re-opened. Persistent symptoms with no answer almost always mean the diagnosis is incomplete.
Living Well
Day-to-day measures that help.
Daily saline irrigation, control of indoor allergens, and good sleep hygiene meaningfully reduce day-to-day symptoms for many patients.
Medical therapy, when prescribed, works best when used consistently rather than as needed — this is one of the most common reasons treatment seems to fail.
In Their Words
From patients of the practice.
I had crusting and whistling that had become part of my daily life. After the repair, things are much calmer and more comfortable. I'm grateful I finally addressed it.
My septal perforation made me anxious because I didn't know what could actually be done. The explanation was clear and realistic, which helped a lot. I felt taken seriously from the start.
I had seen a few doctors before and still felt confused. This was the first visit where the plan made sense to me. My symptoms have improved, and I'm glad I moved forward.
I traveled to New York because septal perforation repair felt too specialized to choose casually. The process was careful, and expectations were explained honestly. I felt very well cared for.
Individual experiences. Results and recovery vary by patient. Testimonials shared with written consent.
Frequently Asked
Patient questions, honestly answered.
Repairability is decided after an in‑office endoscopic exam that documents defect size, edge mobility, and mucosal quality. He reviews prior operative notes and imaging to assess scarring and available septal cartilage. Controlled systemic disease, absence of active intranasal irritants, and sufficient local tissue for tension‑free closure are required for elective repair. When tissue is inadequate, he discusses staged reconstruction or prosthetic options.
The Most Important Step
Get an expert evaluation.
A careful evaluation by a double board-certified physician is the right first step. The conversation is unhurried, the diagnosis is honest, and treatment is matched to what you actually have.