Double Board Certified · Mid-Face Contouring
Cheek Augmentation — structure, projection, definition.
Cheek augmentation restores or enhances mid-face projection — through implants, fat transfer, or carefully-placed injectables. The right choice depends on…
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"The cheekbone is the architectural anchor of the upper face. When it is well-supported, every other feature looks better."
A Note from Dr. Mourad
"Cheek augmentation restores or enhances mid-face projection — through implants, fat transfer, or carefully-placed injectables. The right choice depends on what the underlying bone provides and how much change is wanted."
— Dr. Moustafa Mourad, MD
Overview
What is cheek augmentation?
Cheek augmentation is a procedure that increases the projection, definition, or volume of the mid-face. It can be performed surgically with a precisely shaped cheek implant placed over the malar bone through small intraoral incisions, or with autologous fat grafting in which the patient's own fat is harvested, processed, and transferred to the cheek.
Patients consider cheek augmentation when the mid-face is naturally flat or has lost volume over time, when there is a hollow under the eye or along the cheekbone, or when better facial balance is desired between the upper, mid, and lower face. The aim is structural restoration — not an overdone, gym-shaped cheek.
Implant augmentation is durable and predictable for changing the underlying scaffold of the cheek; fat grafting is well suited to softer volume restoration and can be layered with surgery when both shape and volume are needed.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
01 · Why Dr. Mourad
Diagnosis first, then a plan that fits.
Dr. Mourad evaluates the cheek in the context of the whole face — chin, jawline, and orbital rim — never in isolation.
Augmentation options range from precise injectable contouring to permanent implant placement; the recommendation is matched to the goal and the timeline.
Implants are placed through hidden intra-oral incisions with precise sub-periosteal pocket dissection.
02 · Ideal Candidates
Who benefits most from this operation.
Candidacy is determined together at consultation. The most satisfied patients share three things in common.
I
Flat or Receding Mid-Face
Patients with naturally flat zygomatic projection seeking more defined cheek structure.
II
Age-Related Volume Loss
Patients whose mid-face volume has decreased with age, seeking restoration of youthful contour.
III
Comprehensive Facial Balance
Patients pursuing overall facial balance — often paired with chin or jawline refinement.
Before & After
Real results, real patients.
Every case is unique — tailored to individual anatomy and goals. Browse representative outcomes from the Manhattan practice.
If this describes you, the next step is a quiet, unhurried conversation — not a sales call.
An Honest Note
When this operation may not be right for you.
Patients seeking dramatic, non-anatomic projection are better served by careful counseling and a more measured plan.
Patients with unrealistic expectations of how a single procedure will transform the whole face benefit from a longer consultation.
Patients with active dental infection or unhealthy oral mucosa should defer until those are addressed.
Smokers and patients on certain medications need a planned optimisation window.
03 · Approaches
Three paths to cheek definition.
Cheek augmentation is not a single operation. The right answer depends on whether the change you want is structural, volumetric, or a contour adjustment that should remain reversible.
1 of 3 · Cheek Implant Augmentation
04 · Technique
Implant vs fat transfer.
The two definitive options for lasting cheek augmentation. Each suits a different patient and a different aesthetic goal.
Implant
Permanent structural projection
A silicone implant is placed against the malar bone through a hidden intra-oral incision and secured to maintain stable position. The change is immediate, definitive, and permanent.
Implants are the right choice when the goal is significant projection of a flat or under-developed mid-face — and when the patient wants a single operation with a one-time recovery.
Fat
Soft autologous volume
Fat is harvested from the abdomen or flanks, processed, and re-injected into the mid-face in small aliquots. The result is soft, natural-feeling volume.
Best suited to age-related volume loss and patients who prefer a biologic solution. A portion of grafted fat will not survive, so modest over-correction is planned.
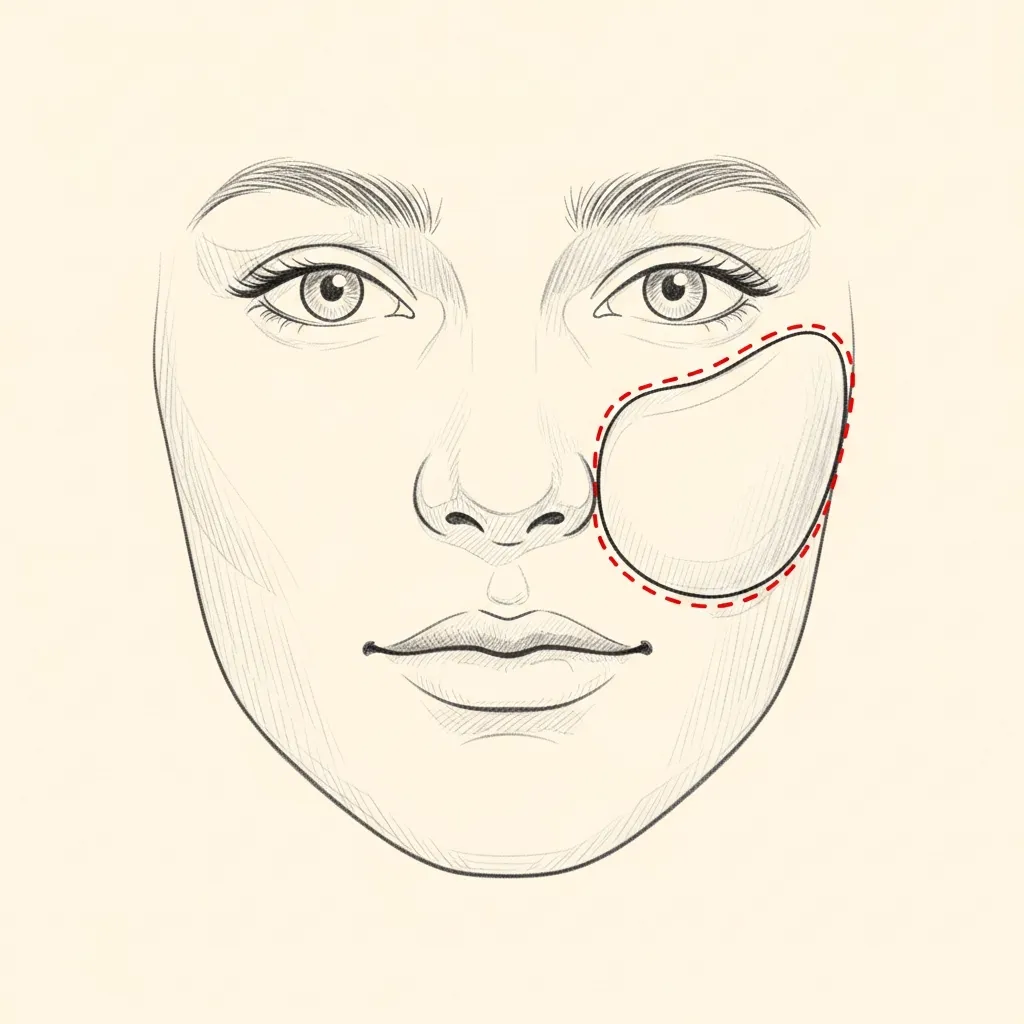
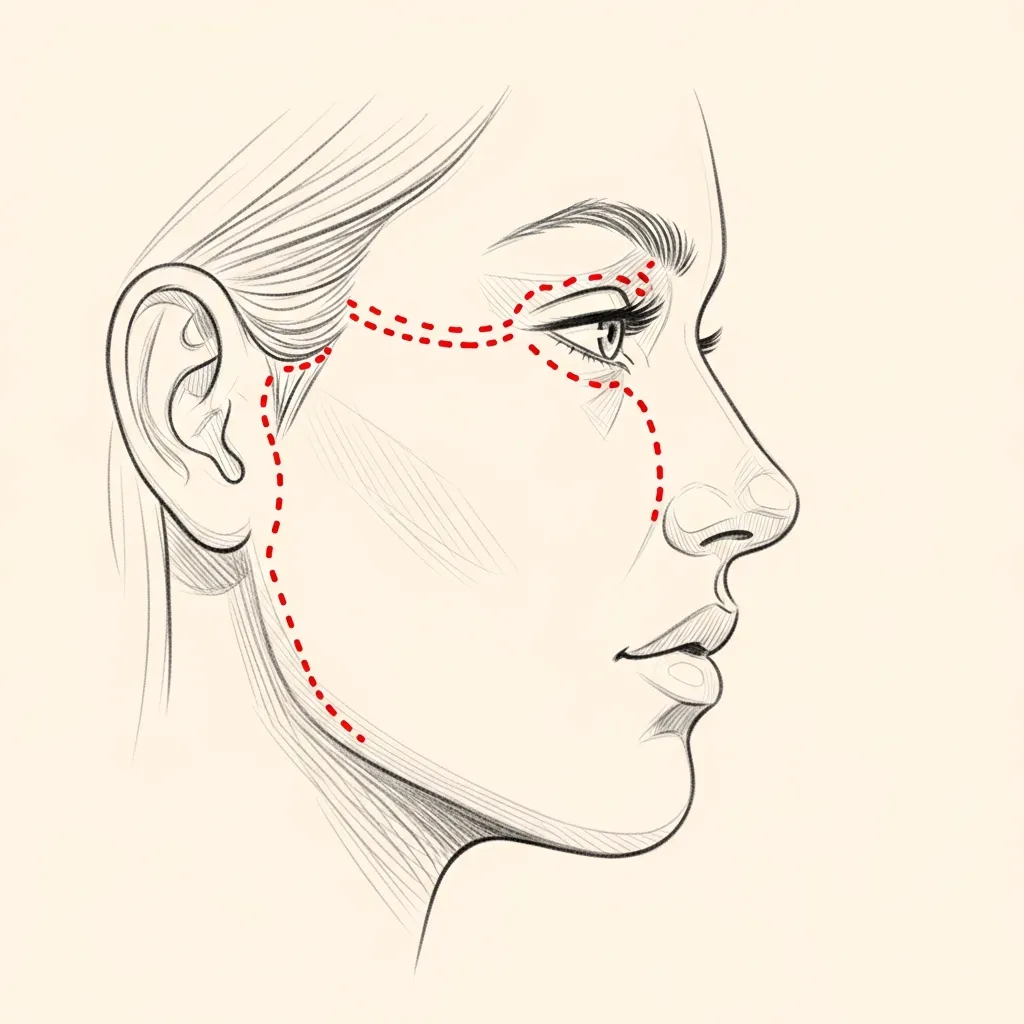
Illustrative diagrams. The right approach is determined together based on starting anatomy and aesthetic goal.
Begin the conversation
A careful, honest evaluation is the right first step.
Cost, Financing & Insurance
Cheek Augmentation Cost, Financing & Insurance in NYC
Cheek augmentation cost depends on the technique selected, whether implants or other methods are used, whether it is combined with other facial procedures, the type of anesthesia, and the surgical setting. Each plan is individualized after facial evaluation.
Cheek augmentation is a cosmetic procedure and is typically self-pay. After consultation, our office provides a personalized estimate based on the recommended plan. Financing may be available for qualified patients through third-party healthcare financing providers.
What May Affect Cost
- Augmentation technique used
- Whether implants are used
- Whether combined with other procedures
- Type of anesthesia
- Surgical setting
- Postoperative care
This information is educational and is not a guarantee of pricing, insurance coverage, reimbursement, financing approval, or surgical candidacy. A personalized estimate is provided after consultation. Insurance coverage depends on the patient’s plan, medical necessity, documentation, and carrier requirements. Financing terms are determined by third-party financing providers.
06 · Recovery
What healing actually looks like.
Stage 01
First 24 Hours
Initial recovery focuses on rest, hydration, and following all post-operative instructions exactly. Pain is managed with multi-modal non-narcotic protocols where appropriate.
Stage 02
Week 1
Swelling and bruising peak in the first few days and improve steadily through the first week. Most patients are presentable for casual social activity by the end of week two.
Stage 03
Weeks 2 – 4
Through weeks two to four the early result begins to settle. Light cardio resumes around three weeks; vigorous exertion and contact activities are deferred per the operative plan.
Stage 04
Months 1 – 6
The final refined result emerges progressively over the following months as residual swelling continues to resolve. Follow-up visits are scheduled across the first year.
Have a specific question?
Send a brief note describing your anatomy or concerns — the office will route it directly to Dr. Mourad for review.

Before You Arrive
Your consultation, prepared.
Bring photographs relevant to your concern, when available.
Bring records from any prior surgery, when available.
List current medications, supplements, and blood-thinning agents.
Note any prior anesthesia issues or chronic medical conditions.
Allow 60 minutes for the first consultation.
Bring questions; no decisions are made at the first visit.
Frequently Asked
Patient questions, honestly answered.
We assess skeletal projection, soft‑tissue volume, and skin quality. If the underlying zygoma is flat or the infraorbital rim lacks support, skeletal augmentation (implant or structural fat graft) is favored. If soft‑tissue volume loss predominates with good skin elasticity, fillers or fat grafting may suffice. Prior surgery, scar tissue, and facial animation are also reviewed before recommending a technique.
Increasing midface projection can lift the nasolabial fold and restore perceived jawline definition by changing the relationship between cheek and mandible. Proper vectoring avoids unwanted fullness in the buccal region and maintains natural transition zones. Overprojection can exaggerate lower‑face shadows; judgment about projection is essential. We evaluate chin position and often discuss concurrent lower‑face procedures for overall balance.
Implants are considered when skeletal support is the primary deficit or when predictable, long‑term projection is required. Fat grafting is preferred for patients desiring autologous tissue, simultaneous correction of adjacent hollows, or modest augmentation. Patients with prior extensive midface scarring or infection risk require individualized planning. Final candidacy is determined in clinic with physical exam and imaging.
After hyaluronic fillers, most swelling and ecchymosis resolve within 24–72 hours, though subtle fullness may last longer. Fat grafting typically produces 5–14 days of visible swelling with social downtime often under two weeks. Surgical implants usually cause most noticeable swelling for 10–14 days, with gradual improvement over several weeks. Individual healing varies with anesthesia type, operative extent, and patient factors.
Malar implants are most often placed through intraoral incisions inside the mouth beneath the upper lip, which leaves no external scar. Some approaches use a lower eyelid incision when concurrent eyelid surgery is planned; in that case, incisions are placed in natural creases. Implant position is secured to minimize migration and to respect the facial animation vectors. Scars are typically well‑concealed when standard approaches are used.
Yes — prior fillers can create palpable nodules or interfere with implant seating; knowledge of product type and timing is important. Recent injectable treatments may require delay before surgery to allow tissue settling. Fat grafting history informs expectations for additional retention and contour changes. We review prior treatment records and may obtain imaging to guide safe planning.
Risks common to all options include asymmetry, contour irregularity, and infection. Fillers carry rare but serious risks such as vascular occlusion and delayed nodules; prompt recognition is essential. Fat grafting can experience partial resorption, oil cysts, or fat necrosis. Implants pose risks of malposition, extrusion, or long‑term palpability; all risks are discussed during consent and managed aggressively if they occur.
Conservative intraoperative sizing and stepwise augmentation minimize overprojection. For implants, we trial different dimensions and observe animation with the patient awake if possible. For fillers and fat grafting, layering and supraperiosteal placement reduce superficial bulking. The reconstructive approach prioritizes vectors that harmonize with skeletal anatomy rather than creating isolated fullness.
Yes, combining procedures is common when structural and soft‑tissue concerns coexist. Fat grafting is frequently paired with facelift to restore volume while addressing descent. Implants can be coordinated with blepharoplasty when both skeletal support and lid contour are being addressed. Combined procedures influence anesthesia choice, operative time, and recovery and are planned during the consultation.
Expect a focused anatomic assessment, photographic analysis, and discussion of goals relative to your skeletal framework. We review prior treatments, medical history, and testing needs. Surgical candidates receive detailed planning including implant options or grafting strategy and a recovery timeline. Final recommendations are individualized and confirmed in person before scheduling.
The Most Important Step
Your expert consultation.
A careful evaluation by a double board-certified physician is the right first step. The conversation is unhurried, the diagnosis is honest, and the operative plan is built around what your anatomy can sustain and what you actually want.