Double Board Certified · AAFPRS Fellowship Director
Facelift in NYC — restore structure, never erase identity.
Dr. Moustafa Mourad performs deep plane facelift surgery in Manhattan, emphasizing anatomic support, individualized planning, and durable contouring.
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"The goal is to look rested, not redone."
Before & After
Facelift results from the practice.

Facelift + Neck Lift · 50s · Female

Facelift · 50s · Female

Facelift + Neck Lift + Blepharoplasty · 50s · Female

Facelift + Neck Lift + Rhinoplasty · 50s · Female

Facelift + Neck Lift · 60s · Male

Revision Facelift + Neck Lift · 70s · Female
Pre and post-operative comparison · Photographed in standardized studio conditions · Written consent on file · Individual results vary
A Note from Dr. Mourad
"In my Manhattan practice, the most common fear I hear is looking ‘done.’ The modern facelift is a structural operation — repositioning the deep tissues, not pulling skin tight. Done well, it returns the face to where it once was, without ever announcing itself."
— Dr. Moustafa Mourad, MD
Medically reviewed by Moustafa Mourad, MD, FACS — dual board-certified Facial Plastic & Reconstructive Surgeon and Otolaryngologist (Head & Neck Surgery).
Last reviewed: June 2026
Is this the right page for you?
This page is for
- You have visible jowling, a softening jawline, or midface descent and are weighing surgery.
- You want to understand how a deep plane facelift differs from a SMAS or mini facelift.
- You are researching a natural, structural result rather than a tight, pulled appearance.
You may be looking for
- Concerns limited to the neck and jawline — see the neck lift page.
- Non-surgical options for early or mild changes — explore MediSpa by NOURA.
- Correcting an unsatisfactory prior facelift — revision facelift is evaluated individually at consultation.
Key takeaways
- A facelift (rhytidectomy) repositions the deeper tissues of the lower face and neck, then removes redundant skin.
- The lasting work happens at the SMAS — the support layer beneath the skin — not skin tightening.
- A deep plane facelift frees the retaining ligaments and lifts the SMAS, fat, and skin together as one unit.
- A SMAS facelift folds or overlaps the SMAS layer and suits moderate jawline laxity.
- A neck lift accompanies almost every facelift, since the jowls and neck are the same problem.
Overview
What is a facelift?
A facelift — known medically as a rhytidectomy — is a surgical procedure that repositions the deeper soft tissues of the lower face and neck and removes the redundant skin that has resulted from years of gravity and volume change. It is designed to address the jowls, the jawline, the upper neck, and the cheek hollows in a single, anatomically planned operation.
A modern facelift is not a skin-tightening procedure. The lasting work happens at the level of the SMAS — the connective tissue layer beneath the skin — which is lifted, repositioned, and secured so the face holds its shape over time. Skin is then redraped without tension, which is what allows incisions to heal as fine lines along the natural creases of the ear.
Patients typically consider a facelift when softening, descent, or jowling of the lower face and neck begins to read on the face from a normal social distance, and when injectables and energy-based treatments are no longer producing the change they once did.
Will a facelift look natural?
A modern facelift repositions the deeper layers of the face rather than simply pulling the skin. That approach is what makes a natural, unpulled result the goal, with the specific technique matched to your anatomy at consultation.
Because faces age differently, the plan is individualized — the aim is to look rested and like yourself, not to change your features.
Do I need a facelift or a neck lift?
It depends on where the laxity is. Jowling and descent of the midface point toward a facelift; loose skin, banding, or fullness under the chin point toward a neck lift — and because the two areas age together, they are frequently addressed in one combined procedure.
An in-person examination of skin quality, muscle banding, and the position of the deeper tissues is what determines the right scope — not age or photographs alone.
Neck lift in NYCWhat is the difference between a facelift and non-surgical tightening?
Non-surgical devices — radiofrequency, ultrasound, and similar energy treatments — stimulate the skin and can produce modest tightening in patients with early, mild laxity. A facelift repositions the deeper structural layers of the face, which no energy device can do; established jowling and significant laxity are surgical problems.
Non-surgical options can be reasonable for maintenance or early changes, and an honest evaluation includes saying when a device is unlikely to meet the goal.
Meet Dr. Mourad
A facelift surgeon in NYC focused on structure, restraint, and results that do not look pulled.
Dr. Moustafa Mourad is a dual board-certified facial plastic and reconstructive surgeon whose practice is dedicated to surgery of the face, nose, sinuses, and neck. For facelift patients in NYC, his background in facial plastic surgery, head and neck anatomy, reconstruction, and fellowship-level teaching shapes the way he evaluates facial aging. The goal is not to tighten skin for the sake of tightness; it is to restore structure in a way that looks natural at rest, in expression, and over time.
His facelift planning draws on that same structural philosophy. He evaluates the cheeks, jowls, jawline, neck, platysma, skin quality, prior filler, facial asymmetry, hairline, ear shape, and scar placement before recommending a facelift, deep-plane facelift, SMAS approach, neck lift, or a more conservative alternative.
His aesthetic philosophy is deliberately restrained. A good facelift should not advertise itself. It should improve the jawline, soften jowls, restore support, and refresh the neck without creating an over-tightened face, distorted earlobes, a pulled mouth, or a hairline that looks surgically altered. Consultations focus on explaining what the operation can improve, what it cannot improve, and when a less invasive or staged plan may be more appropriate.
- Dual board-certified facial plastic and reconstructive surgeon
- Teaches facelift and facial plastic surgery principles through the AAFPRS fellowship
- Focus on structural support rather than skin tension
- Natural, identity-preserving facelift philosophy
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
01 · Why Dr. Mourad
A surgeon other surgeons trust with their hardest cases.
Dr. Moustafa Mourad structures the consultation around anatomy rather than a procedure checklist. Clinical photographs document frontal, profile, and oblique views at rest and with animation. He evaluates malar projection, mandibular contour, platysmal banding, and the location of retaining ligament laxity to determine optimal vectors of lift. Dynamic tests of facial movement help predict how repositioned tissues will drape, which informs decisions about vertical versus lateral vectoring and the extent of deep dissection required.
The medical and procedural history is reviewed in detail, including prior facial surgery and injectable filler use. Medication reconciliation screens for anticoagulants and supplements that influence bleeding risk. When prior operative reports are available, Dr. Mourad reviews them to anticipate scar planes and altered anatomy. He documents findings with standardized photos and uses them to discuss realistic goals, incision patterns, and the need for adjunctive procedures like fat grafting or cheek augmentation to restore midface projection.
Surgical plans emphasize reconstruction principles: precise hemostasis, preservation of vascular pedicles, and layered closure to protect skin perfusion. When neck contour is a concern, Dr. Mourad discusses platysmaplasty and neck lift NYC criteria, integrating neck decisions into a single, harmonious plan when appropriate. He outlines perioperative steps, expected operative time, anesthesia choices, and postoperative milestones so patients understand the recovery timeline before consenting to surgery.
02 · Ideal Candidates
Who benefits most from a facelift.
A facelift is a structural restoration — it returns the deep tissues of the face to where they once were. The best candidates have noticeable lower-face descent and the health to recover well from an outpatient operation under general anesthesia.
I
Lower Face Laxity
Visible jowling along the jawline, descent of the cheek fat pad, and softening of the cervicomental angle — classic signs of the SMAS layer descending with time.
II
Folds & Marionette Lines
Deepening nasolabial folds and marionette lines that no longer respond to soft-tissue filler alone — when volume restoration has reached its limit and structural elevation is the right next step.
III
Healthy & Realistic
Non-smokers in good overall health, with realistic expectations about what a facelift does and does not do. The procedure restores structure; it does not change the underlying skin quality.
Before & After
Facelift and Neck Lift Before and After Cases
Documented facelift and neck lift outcomes from the Manhattan practice, photographed in standardized studio conditions. Each case is shown with written consent on file. Individual results vary with anatomy and goals.

Facelift + Neck Lift · 50s · Female
Facelift combined with a neck lift for a female patient in her 50s to address midface and jawline laxity along with submental and neck fullness. Documented in frontal, oblique, and lateral views before and after surgery; photographed in standardized studio conditions with written consent on file.

Facelift + Neck Lift + Rhinoplasty · 50s · Female
Facelift combined with a neck lift and rhinoplasty for a female patient in her 50s to address midface and jawline laxity, submental and neck fullness, and nasal contour. Documented in frontal, oblique, and lateral views before and after surgery; photographed in standardized studio conditions with written consent on file.
Facelift + Neck Lift + Blepharoplasty · 50s · Female
Facelift combined with a neck lift and blepharoplasty for a female patient in her 50s to address midface and jawline laxity along with periorbital aging. Documented in frontal and oblique views before and after surgery; photographed in standardized studio conditions with written consent on file.

Facelift + Neck Lift · 60s · Male
Facelift combined with a neck lift for a male patient in his 60s to address midface, jawline, and neck laxity. Documented in oblique and lateral views before and after surgery; photographed in standardized studio conditions with written consent on file.
Pre and post-operative comparison · Photographed in standardized studio conditions · Written consent on file
If this describes you, the next step is a quiet, unhurried conversation — not a sales call.
An Honest Note
When a facelift may not be right for you.
If your concerns are primarily about skin texture, fine lines, or pigmentation — resurfacing, peels, or energy-based treatments may serve you better than surgery.
Active smokers face significantly elevated risk of skin necrosis and impaired healing. A formal nicotine-free window before surgery is non-negotiable.
Patients in their early thirties with very mild changes are often better served by less-invasive options. A facelift is not a preventive operation.
Unstable medical conditions — uncontrolled blood pressure, untreated sleep apnea, bleeding disorders — must be addressed before any elective facial surgery.
03 · Approaches
Six paths to facial rejuvenation.
A facelift is not a single operation. Each variant addresses a different anatomy, age range, or set of goals. Browse the editions below to see how each technique is considered, who it suits, and how it relates to the others.
1 of 6 · Deep Plane Facelift
04 · Technique
Deep plane vs SMAS facelift.
The two dominant modern facelift techniques differ in where the surgical plane sits. The right choice depends on the anatomy of the face, the degree of descent, and the goals of the patient.
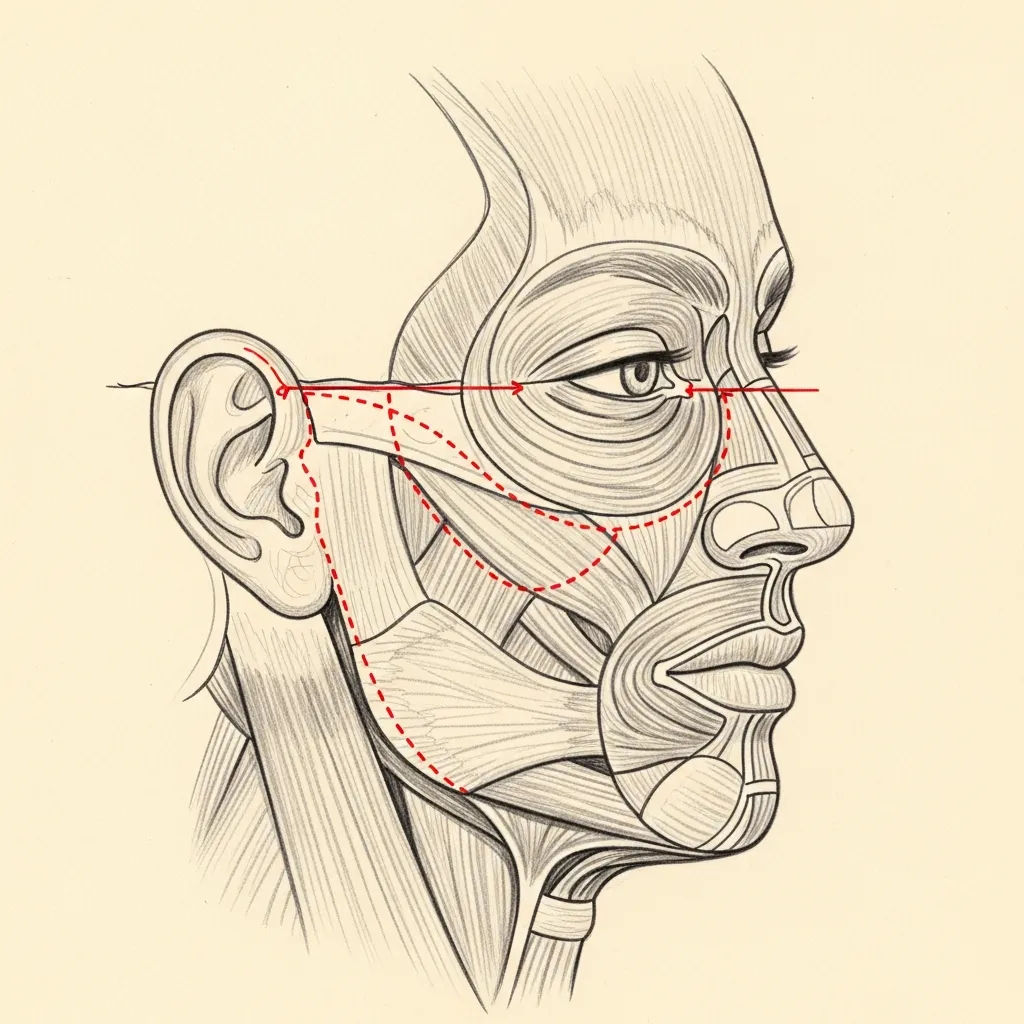
Deep Plane
Beneath the SMAS
The deep plane facelift releases the retaining ligaments of the face and elevates the SMAS, fat, and skin together as one composite unit. Because the layers are not separated, the result is unusually natural and the vector of elevation is true.
This technique addresses the midface, nasolabial fold, jowl, and upper neck in a single coordinated movement. It is the technique of choice for patients with significant midface descent.
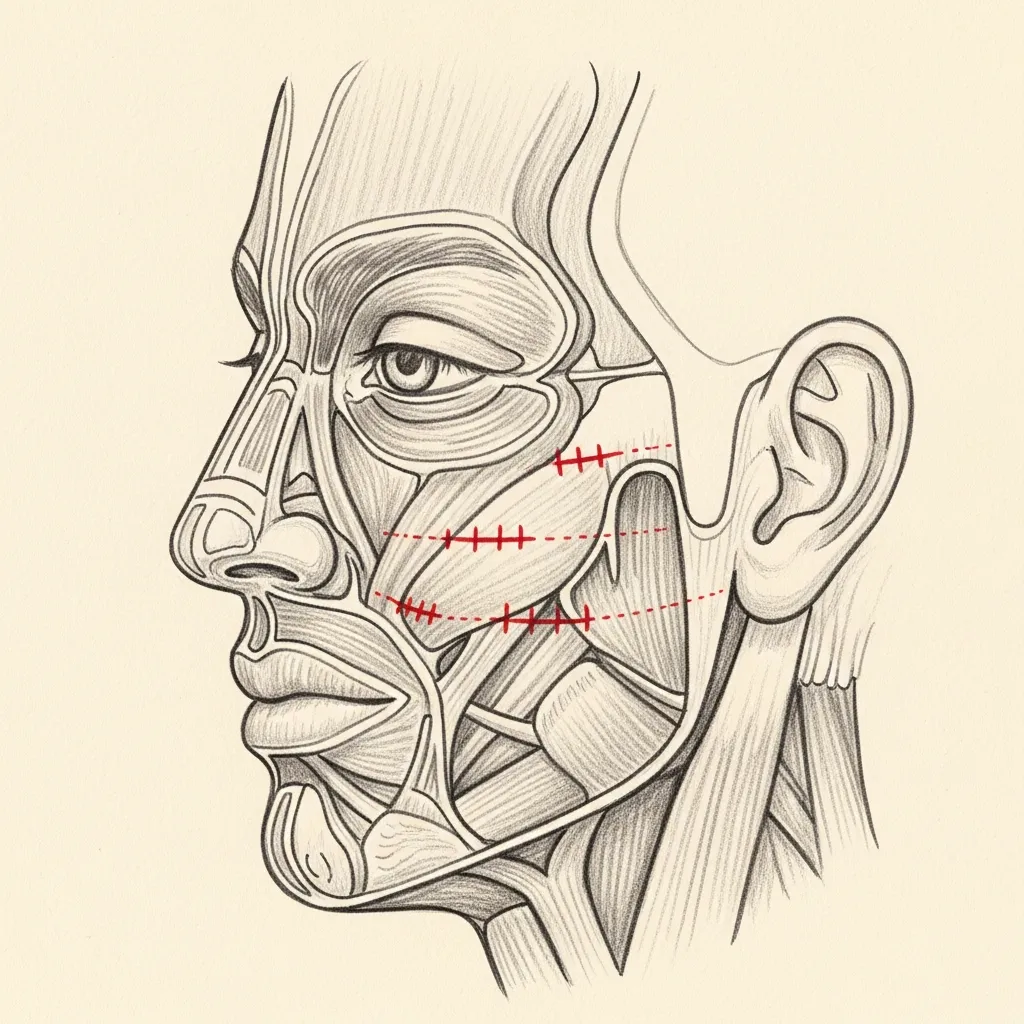
SMAS
Plication or Imbrication
A SMAS facelift tightens the SMAS layer through folding (plication) or overlapping (imbrication) without sub-SMAS dissection. It is a robust, predictable operation with a strong safety profile.
It is well suited to patients with moderate jawline laxity who do not require deep midface release. Recovery can be slightly faster because the dissection planes are more limited.
Illustrative diagrams. The appropriate plane is determined individually at consultation based on anatomy and goals.
Begin the conversation
A consultation is a clinical evaluation — not a sales conversation.
Cost, Financing & Insurance
Facelift Cost, Financing & Insurance in NYC
The cost of a facelift in NYC varies because every surgical plan is individualized. A mini facelift, lower facelift, deep plane facelift, revision facelift, or combined face and neck lift may involve different levels of surgical complexity, operating time, anesthesia, facility needs, and postoperative care.
Facelift surgery is generally considered cosmetic and is typically self-pay. During consultation, Dr. Mourad can evaluate your facial anatomy, discuss your goals, and provide a personalized quote based on the recommended surgical plan. Financing options may be available for qualified patients through third-party healthcare financing providers.
What May Affect Cost
- Type of facelift performed
- Degree of facial laxity
- Whether the neck is treated at the same time
- Primary vs revision surgery
- Anesthesia and facility fees
- Postoperative care
This information is educational and is not a guarantee of pricing, insurance coverage, reimbursement, financing approval, or surgical candidacy. A personalized estimate is provided after consultation. Insurance coverage depends on the patient’s plan, medical necessity, documentation, and carrier requirements. Financing terms are determined by third-party financing providers.
05 · In Dr. Mourad's Words
The facelift, explained.
Dr. Mourad on the modern facelift — the philosophy, the technique, and what a natural, structural result really means.
The Modern Facelift
Dr. Mourad discusses how a deep plane facelift repositions the deeper tissues of the face — restoring structure rather than pulling skin tight.
06 · Recovery
What healing actually looks like.
Stage 01
First 24 Hours
The first 24 hours involve a soft compressive dressing, head elevation, and rest. Discomfort is generally moderate and well controlled with non-narcotic medications. Drains, when used, are typically removed within a day or two.
Stage 02
Week 1
Through the first week, bruising and swelling peak around day three and begin to subside. Sutures in front of the ear are removed at day seven. Most patients are presentable for quiet social return at ten to fourteen days.
Stage 03
Weeks 2 – 4
Between weeks two and four, residual swelling steadily declines. Light makeup covers most residual discoloration. Light cardio resumes around three weeks; strength training is delayed further.
Stage 04
Months 1 – 12
From one to twelve months, the deep tissues continue to settle. Final contour and scar maturation are appreciated by six to twelve months. The result tends to look more natural with each passing month.
Have a specific question?
Send a brief note describing your anatomy or concerns — the office will route it directly to Dr. Mourad for review.
Long-term
How a facelift relates to other procedures.
A facelift repositions the deeper tissues of the cheek, jowl, and jawline. When midface volume has been lost, structural support through cheek augmentation may be discussed as a complementary step, since restoring midface projection can soften the appearance of jowling.
Laxity of the neck is addressed at the same time in most cases. When prominent platysma bands and an obtuse neck angle are present, a neck lift treats the muscle and submental fullness that a facelift alone does not reach.

Investment
Understanding the value.
A facelift is a meaningful investment. The fee reflects the surgeon's experience, an accredited operating facility, board-certified anesthesia, and a structured year of follow-up care.
The right operation, performed once and well, almost always proves to be the better long-term value than a series of smaller interventions that drift over time.

Before You Arrive
Your consultation, prepared.
Bring photographs of your face from your 30s and 40s if you have them.
Note any prior facial surgery, injectable history, or facial trauma.
List current medications, supplements, and any blood-thinning agents.
Allow 60 minutes; expect a thorough physical examination of the face and neck.
Bring questions. Consultations are designed for a real conversation.
No decisions are made at the first visit — that is by design.
Patient Reviews
Facelift Patient Experiences
Selected public patient reviews. Individual experiences vary.
“My results are natural and stunning.”
Real patient experiences
Selected public reviews from patients of the practice.
Your privacy matters
We never share personal health information.
Board-certified expertise
Dual board-certified facial plastic and reconstructive surgeon.
Individual results vary. Reviews reflect individual experiences and are not a guarantee of outcome.
At a Glance
Facelift fact snapshot.
- Treats
- Jowling, descent of the midface, deep folds around the mouth, and loose skin of the lower face — often together with the neck.
- Does not treat
- Skin texture, sun damage, pigment, or volume loss on their own — those are managed with skin treatments or volume restoration, sometimes alongside surgery.
- Evaluation
- In-person examination of skin quality, deeper tissue position, muscle banding, and bone structure, with a plan matched to how your face has aged.
- Related conditions
- Neck laxity and platysmal banding, brow descent, volume loss of the midface.
- Possible combined procedures
- Neck lift, deep plane technique, fat transfer, brow or eyelid surgery, skin resurfacing.
- Recovery summary
- Most patients are socially presentable in about two weeks; swelling and firmness continue to settle over several months.
- Insurance / functional distinction
- Facelift surgery is cosmetic and self-pay; it is not submitted to insurance.
- When to seek evaluation
- When jowling or facial laxity bothers you in photographs or the mirror, and skincare or devices are no longer meeting the goal.
Why patients trust this practice
Care led by a double board-certified specialist
Double board certified
American Board of Facial Plastic & Reconstructive Surgery and American Board of Otolaryngology — Head & Neck Surgery.
AAFPRS Fellowship Director
Trains fellows through the American Academy of Facial Plastic and Reconstructive Surgery.
Published author
Contributions to the academic literature of facial plastic surgery.
Face, nose & sinus focus
A practice concentrated above the clavicles, including complex revision evaluations.
Frequently Asked
Patient questions, honestly answered.
The decision rests on the pattern of descent and tissue mobility identified on exam and photographs. When midface descent and jowl formation coexist with loss of submalar support, the deep plane permits en bloc mobilization of the malar and jowl complex. For isolated lower‑face laxity with good midface support, an SMAS‑based modification may be appropriate. Final selection is made after in‑person assessment and discussion of tradeoffs.
Recent large‑volume fillers can obscure planes of dissection and increase firmness in tissue, which may alter elevation and redraping. Very old or granulomatous filler deposits can be adherent and require identification before surgery. We document prior treatments and may obtain imaging or plan staged management when filler complicates dissection. The operative approach is adapted to protect tissue perfusion and avoid unexpected planes.
Expected findings include moderate swelling and bruising that peak within 48–72 hours and gradually improve over 10–21 days. Mild numbness and a tight sensation are common and usually resolve over weeks to months. Stable incision edges without progressive discoloration, and steadily decreasing pain controlled by oral medication, indicate routine healing. Any rapidly expanding swelling, severe asymmetry, or increased pain should prompt urgent contact with the surgical team.
Pain is usually moderate and controlled with a short course of oral analgesics, often a combination of acetaminophen and a limited opioid for the first 48–72 hours when needed. Long‑acting local anesthetic blocks or infiltration are used intraoperatively to reduce immediate postoperative discomfort. Most patients taper to only acetaminophen or NSAIDs within the first week. We provide individualized pain plans and clear instructions for safe medication use.
Incisions are placed to follow natural contours: temple lines, the preauricular crease, around the earlobe, and into the postauricular hairline when indicated. This placement minimizes visibility once healed and allows hair to naturally mask transition zones. Scar appearance depends on wound handling, patient biology, and postoperative care; we discuss scar management strategies preoperatively, including topical care and, if needed, later refinement. Concealment is an explicit element of incision design.
Revision cases present altered scar planes, reduced tissue mobility, and variable blood supply; these factors complicate dissection and lengthen operative time. Scar tissue increases the risk of skin edge tension and may raise the likelihood of delayed healing or contour irregularity. Nerve identification can be more challenging and the plan is frequently more conservative with staged adjuncts such as fat grafting. Preoperative mapping and review of prior operative notes are essential for safe planning.
Combining procedures is possible for selected patients and is decided after careful medical review and photographic planning. Combined operations increase operative time and influence recovery expectations; they are appropriate only when overall health and anesthetic risk permit. Concurrent procedures may offer unified anesthetic and recovery efficiency but require coordinated planning about vectors of rejuvenation. A discussion of risks, benefits, and staging options occurs at consultation.
Most patients see major contour improvement by 3 months as swelling subsides and soft tissues settle. Continued refinement occurs between 6 and 12 months as scar remodeling and tissue relaxation progress. Nerve‑related changes and residual mild swelling can persist longer in some areas. We schedule follow‑up visits to document progress and advise on adjunctive measures if contour irregularities remain after 6–12 months.
Drains are used selectively based on intraoperative bleeding and the extent of dissection; many deep plane cases use short‑term drains when indicated. When placed, drains are typically removed within 24–48 hours once output falls below a measured threshold. Dressing instructions and drain care are reviewed before discharge and a nurse removes drains in clinic. Use of drains is individualized to minimize hematoma risk while balancing patient comfort.
Typical follow‑up includes a 24–72 hour early check, a 1‑week visit for incision and dressing review, a 2–3 week visit for suture and aesthetic assessment, then 3‑month and 6‑ to 12‑month reviews to track settling. Additional visits are scheduled sooner if concerns arise. Long‑term annual reviews are available to counsel on maintenance and address late changes. All follow‑up timing is tailored to healing progress and any adjunctive procedures.
Major risks include hematoma, wound healing problems, infection, sensory changes, and temporary facial nerve weakness; permanent nerve injury is uncommon. Hematoma most often presents in the first 24–48 hours and may need urgent evacuation to protect skin perfusion (see AAFPRS patient resources: https://www.aafprs.org/patient-resources/). Early recognition of skin edge compromise or expanding pain prompts immediate assessment. We review emergency protocols at preoperative visits and maintain low thresholds for intervention.
Durability depends on patient age, skin quality, genetics, and the extent of structural support restored; meaningful contour improvement commonly endures for several years rather than decades. Techniques that restore deep ligamentous support and address the platysma typically offer longer maintenance than skin‑only approaches (see ABFPRS patient information: https://www.abfprs.org/). Ongoing sun protection, skin care, and periodic non‑surgical maintenance can prolong results. Exact duration varies and is discussed at consultation.
Clinical references
This page draws on published clinical practice guidelines and public-health references. These sources inform general patient education and do not replace an individual evaluation with Dr. Mourad.
- 01American Society of Plastic Surgeons. Facelift (Rhytidectomy): procedure, candidacy, and recovery overview. ASPS
- 02American Academy of Facial Plastic and Reconstructive Surgery. Patient resources on facial plastic surgery procedures. AAFPRS
- 03U.S. National Library of Medicine (MedlinePlus). Plastic and Cosmetic Surgery. MedlinePlus
Explore Further
Related procedures & resources
A facelift is often planned alongside complementary procedures of the neck and upper face. These pages explain how the work relates.
Deep Plane Facelift
A sub-SMAS release of the retaining ligaments for midface descent and deeper folds.
Read moreSMAS Facelift
Tightens the SMAS layer through plication or imbrication for moderate jawline laxity.
Read moreMini Facelift
A shorter-incision, limited-dissection lift for early jowling in the right candidate.
Read moreRevision Facelift
Correction of an unsatisfactory or overdone prior facelift, focused on natural contour.
Read moreMale Facelift
Facelift surgery planned for male anatomy, beard-bearing skin, and incision placement.
Read moreJawline & Jowl Rejuvenation
Surgical and structural approaches to a softened jawline and jowls.
Read moreNeck Lift
Almost always combined with a facelift to restore the jawline and cervicomental angle.
Read moreDeep Plane vs SMAS Facelift
How the two main techniques differ, and which tends to suit which anatomy.
Read moreFacelift Recovery Timeline
A realistic, week-by-week look at what healing involves.
Read moreBefore & After Gallery
Representative facelift and neck lift cases, photographed with written consent on file.
Read morePatient Reviews
Read experiences from patients of the practice.
Read moreRequest a Consultation
Begin with an unhurried clinical evaluation.
Read moreThe Most Important Step
Your expert consultation.
A facelift consultation is a careful clinical evaluation of facial anatomy and goals. The visit is unhurried, the conversation is honest, and any surgical plan is built around the patient — never the other way around.