Double Board Certified · Specialized Revision Practice
Revision Rhinoplasty NYC — Correct, Rebuild, Restore
Dr. Moustafa Mourad performs revision rhinoplasty in NYC for patients who remain unhappy with the appearance, structure, or breathing of the nose after prior nasal surgery. Revision surgery may involve scar release, cartilage grafting, septal reconstruction, nasal valve repair, and careful reshaping to restore natural balance and durable support.
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"The hardest cases are the ones I am sent."
Before & After
Rhinoplasty results from the practice.

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty · 20s · Female

Revision Rhinoplasty · 30s · Male

Ethnic Rhinoplasty · 40s · Male

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty · 40s · Female

Primary Rhinoplasty · 30s · Female

Ethnic Rhinoplasty · 30s · Male

Primary Rhinoplasty + Sinus Surgery · 40s · Female

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty + Sinus Surgery · 20s · Female

Primary Rhinoplasty · 30s · Female

Primary Rhinoplasty · 50s · Male

Primary Rhinoplasty + Sliding Genioplasty · 20s · Male

Revision Rhinoplasty + Sinus Surgery · 30s · Male

Ethnic Rhinoplasty · 20s · Male

Primary Rhinoplasty + Sinus Surgery · 20s · Female

Ethnic Rhinoplasty + Sinus Surgery + Broken Nose Repair · 30s · Female

Revision Rhinoplasty · 20s · Female
Primary Rhinoplasty + Broken Nose Repair · 20s · Female

Revision Rhinoplasty · 30s · Female

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty + Neck Lift · 30s · Female

Revision Rhinoplasty · 30s · Female

Revision Rhinoplasty · 40s · Female

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty · 20s · Male

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty · 20s · Female

Facelift + Neck Lift + Rhinoplasty · 50s · Female

Revision Rhinoplasty · 30s · Female

Primary Rhinoplasty + Broken Nose Repair · 20s · Female

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty · 20s · Female
Pre and post-operative comparison · Photographed in standardized studio conditions · Written consent on file · Individual results vary
A Note from Dr. Mourad
"Revision rhinoplasty is a different operation from primary rhinoplasty. The scar tissue is dense, the cartilage is depleted, and the airway has often been compromised. What this work demands is restraint, structural thinking, and a willingness to take cases that others decline."
— Dr. Moustafa Mourad, MD
Medically reviewed by Moustafa Mourad, MD, FACS — dual board-certified Facial Plastic & Reconstructive Surgeon and Otolaryngologist (Head & Neck Surgery).
Last reviewed: June 2026
Make sure you're in the right place
Is this the right page for you?
This page is for
- You have already had one or more nasal surgeries and remain unhappy with the breathing, the appearance, or both.
- You have scar tissue, weakened or depleted cartilage, or a nose that looks or functions differently than planned after prior surgery.
- You were told elsewhere that your case is too complex or inoperable.
You may be looking for
- If you have never had nasal surgery, primary rhinoplasty is the right starting point.
- If your only concern is breathing through a deviated septum, see septoplasty.
- If your nose was recently broken, see broken nose repair.
Key takeaways
- Revision rhinoplasty corrects a nose after prior surgery, where scar tissue and depleted cartilage add complexity.
- Cartilage grafts — from the septum, ear, or rib — rebuild lost support before refinement is possible.
- Timing matters most: tissues should soften and settle, often about twelve months, before re-operating.
- Breathing and appearance are addressed together, since the structural and aesthetic fixes overlap.
- Not every concern can be fully corrected; realistic goals depend on anatomy, scarring, and healing.
Overview
What is revision rhinoplasty?
Revision rhinoplasty is rhinoplasty performed on a nose that has already had previous nasal surgery. Sometimes called secondary rhinoplasty or corrective nose surgery, it is an inherently more complex operation than primary rhinoplasty because the anatomy has been altered, the cartilage stock may be depleted, scar tissue distorts normal tissue planes, and the underlying structural support may be weakened by prior reduction.
Patients pursue revision for many reasons — residual cosmetic concerns, asymmetry, an over-rotated or pinched tip, a saddle deformity, a pollybeak fullness, or new breathing problems that emerged after the first operation. Functional revision and cosmetic revision are frequently performed together because the structural fix and the aesthetic fix are the same operation.
A revision plan often requires cartilage grafting — most commonly from the ear or, when significant rebuilding is needed, from the rib — to restore lost support before refinement is possible. The most important decision is usually when to operate, not how; mature scar tissue and stable healing from the prior surgery are essential before revision.
What makes revision rhinoplasty different from a first operation?
Revision rhinoplasty is surgery on a nose that has already been operated on. Scar tissue, altered anatomy, and reduced cartilage make it more complex than a primary procedure, and rebuilding structural support with cartilage grafts is often part of the plan.
A careful evaluation of what the previous surgery changed — and what tissue remains to work with — comes before any plan, which is why these cases are approached more conservatively than a first rhinoplasty.
When is rib cartilage needed in revision rhinoplasty?
Rib cartilage is generally considered when the septum no longer has enough cartilage to rebuild support — most often after one or more prior surgeries that used or removed septal cartilage. It provides strong, straight grafting material for reconstructing the bridge, tip, or sidewalls.
Whether rib, ear, or remaining septal cartilage is the right source depends on how much structure needs to be rebuilt, which is assessed at consultation and sometimes with imaging.
See a rib-graft caseWhat problems can revision rhinoplasty address?
Revision rhinoplasty can address structural collapse, breathing obstruction, asymmetry, over-resection, a pinched or upturned tip, and irregularities along the bridge from a prior operation. Many revisions combine airway repair with refinement of the external shape.
The realistic scope of a revision depends on the quality of the remaining tissue — some concerns can be improved substantially while others are managed more conservatively.
How long should I wait before revision rhinoplasty?
Most surgeons advise waiting roughly a year after the prior operation before a full revision, because swelling continues to change the nose during that time and operating on inflamed tissue adds risk. Exceptions exist for clear structural problems or significant airway obstruction, which can sometimes be addressed sooner.
The right timing is individualized — an earlier consultation can still be useful to document the anatomy and plan ahead, even if surgery itself waits.
BEST of MANHATTAN
2026
Modern Luxury Best of Manhattan 2026
Rhinoplasty recognition, applied carefully to complex revision planning
Dr. Moustafa Mourad was named "Best Rhinoplasty" in Modern Luxury's Best of Manhattan 2026 medical category. For revision patients, the relevance is not a slogan — it is the same rhinoplasty judgment applied to scar tissue, altered anatomy, airway compromise, and structural rebuilding.
Third-party recognition is not a guarantee of outcome. Every rhinoplasty plan is individualized.
How Dr. Mourad Plans
How Dr. Mourad plans a revision rhinoplasty
Revision planning begins with the patient's story. What was the original goal? What changed after surgery? Did breathing worsen? Did the shape change as swelling resolved? Was there trauma after surgery? Were implants or grafts used? Was there infection, prolonged swelling, filler, or steroid injection?
The next step is photographic review. Old photos can show the original anatomy and help separate preexisting asymmetry from surgery-related changes. Operative reports are valuable because they may reveal whether septal cartilage was removed, whether spreader grafts were placed, whether osteotomies were performed, and whether alloplastic materials or cadaveric cartilage were used.
The examination evaluates both appearance and airway — the bridge, middle vault, tip, nostril rims, alar base, columella, septum, turbinates, internal and external valves, skin thickness, scar density, and cartilage support. Nasal endoscopy may be used to assess the septum, valves, turbinates, perforation, or synechiae.
The surgeon then determines the cartilage inventory. If septal cartilage remains, it may be useful; if not, ear or rib cartilage may be needed. Major support loss, saddle deformity, valve collapse, or multiple prior surgeries often require stronger cartilage than the septum or ear can provide.
The final plan prioritizes safety. Sometimes the patient should wait longer before revision; sometimes staging is safer than attempting every correction at once. In all cases revision is less predictable than first-time rhinoplasty, and improvement — not perfection — is the goal. For context on the operation as a whole, see the rhinoplasty overview.
Implant & Graft Complications
Revision after an implant, cadaveric graft, or prior graft failure
Some revision patients have prior grafts or implants that no longer behave as intended. These may include silicone, Gore-Tex, Medpor, cadaveric rib cartilage, irradiated cartilage, ear cartilage, septal cartilage, or rib cartilage from a previous operation. The problem may be infection, exposure, extrusion, resorption, warping, displacement, contour visibility, skin thinning, or collapse after support weakens.
A prior implant does not automatically mean it must be removed, and a prior cadaveric graft does not automatically mean it failed. The decision depends on symptoms, skin quality, infection risk, stability, contour, breathing, and whether the material is contributing to the problem.
Silicone, Gore-Tex, and Medpor may create special concerns because they are foreign materials. If they become infected, exposed, mobile, or visible through the skin, removal and reconstruction may be needed. In some patients the surrounding soft tissue may be thin or scarred, which can make revision more complex.
Cadaveric rib cartilage can be useful in selected patients, but if it resorbs, warps, shifts, or fails to provide durable support, the nose may need reconstruction with autologous cartilage. Autologous rib cartilage may be preferred when strong structural support is required, especially in major saddle nose repair, severe middle-vault collapse, or revision after multiple prior operations.
The safest plan begins with identifying what is currently in the nose. Operative reports, prior imaging, old photos, and a careful exam all help. Patients should bring any available operative records to consultation.
Timing
When revision should be delayed
Revision rhinoplasty is often delayed until tissues have matured. In many cases, waiting at least twelve months after prior rhinoplasty is preferred because swelling, scar tissue, and skin behavior continue to evolve. Operating too early can increase risk and may lead to overcorrection or unnecessary surgery.
Exceptions may include infection, implant exposure, severe airway compromise, trauma, or urgent complications. These situations require individualized evaluation.
Patients should be cautious about chasing early swelling. Irregularities seen at three or six months may improve. Conversely, true structural collapse or valve compromise may become more obvious as swelling resolves. Timing must be chosen based on anatomy, healing, and risk.
What It Can Address
Revision Rhinoplasty Problem Map
Revision rhinoplasty addresses a defined set of problems left behind by prior nasal surgery. The right plan depends on what was done before and what the tissues will now tolerate. Where a dedicated page exists, each card links to a more detailed explanation.
Pinched tip
A pinched tip may occur when too much lower lateral cartilage has been removed, weakened, or scarred. The nostril rims can look narrow, the tip may appear sharp or collapsed, and the external nasal valve may not support airflow. Revision often requires rebuilding support with cartilage grafts rather than simply reshaping the surface.
Pinched nose after rhinoplasty →Pollybeak deformity
Pollybeak deformity describes fullness in the supratip region, where the area above the tip looks convex or beak-like. It may result from residual cartilage, scar tissue, weak tip support, or disproportion between the bridge and tip. Treatment depends on whether the fullness is scar, cartilage, skin thickness, or structural underprojection.
Pollybeak deformity →Saddle nose deformity
A saddle nose occurs when the bridge loses support and becomes depressed. It may follow septal over-resection, trauma, infection, autoimmune disease, septal perforation, or prior surgery. Revision usually requires structural rebuilding, often with rib cartilage when support loss is significant.
Saddle nose deformity →Inverted-V deformity
An inverted-V deformity can appear when the middle vault collapses after hump reduction or inadequate support of the upper lateral cartilages. Patients may see visible shadowing along the upper nose and may also have internal nasal valve obstruction. Spreader grafts or other middle-vault reconstruction may be needed.
Inverted-V deformity →Alar retraction
Alar retraction occurs when the nostril rim sits too high or pulls upward, creating excessive nostril show or asymmetry. It may result from cartilage over-resection, scar contraction, prior surgery, or weak lower lateral cartilage support. Correction may require alar rim grafts, composite grafts, or structural reconstruction.
Alar retraction →Over-rotated tip
An over-rotated tip may make the nose look too upturned or expose too much nostril. In revision this can be difficult because the skin and scar tissue may resist repositioning. Correction may require tip support, septal extension grafting, or other structural maneuvers.
Residual hump
A residual hump may remain after primary rhinoplasty or become visible after swelling resolves. The cause may be residual bone, cartilage, callus, or imbalance between the radix, dorsum, and tip. Revision should be conservative and precise, because additional dorsal work can affect nasal stability and valve function.
Crooked nose after surgery
A nose may remain crooked or become crooked after surgery because of bone memory, cartilage memory, septal deviation, asymmetric scarring, or incomplete correction of the original deformity. Revision requires identifying whether the deviation is bony, cartilaginous, septal, soft tissue, or facial asymmetry.
Nasal valve collapse
Nasal valve collapse after rhinoplasty may occur when the middle vault or lower lateral cartilages lose support. Patients may notice that nasal strips help, that the sidewall collapses when inhaling, or that breathing worsened after surgery. Treatment may require spreader grafts, batten grafts, lateral crural support, or broader functional revision.
Nasal valve collapse treatment →Septal perforation
A septal perforation is a hole in the septum that may cause crusting, bleeding, whistling, obstruction, or dryness. If present in a revision patient, the perforation must be evaluated carefully before aesthetic or functional revision is planned. Repair may be staged or, in selected cases, combined.
Septal perforation repair →Implant or graft complication
Prior implants, alloplastic materials, cadaveric grafts, or weakened autologous grafts can create later problems such as resorption, infection, extrusion, contour irregularity, skin thinning, or collapse. Treatment depends on the material, surrounding tissue, skin condition, infection risk, and need for replacement support.
Scar tissue & thick skin
Scar tissue can limit how much the skin envelope moves during revision. Thick skin can hide fine definition and hold swelling longer. Revision planning must account for how much change the skin can safely reveal; in some cases restraint is safer than aggressive reshaping.
Not every concern can be fully corrected, and revision outcomes depend on individual anatomy, scarring, and healing. Realistic, individualized goals are discussed in detail during consultation.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
01 · Why Dr. Mourad
A specialist in the cases others won't take.
Dr. Moustafa Mourad begins with an anatomy‑first evaluation that prioritizes structural stability and airway dynamics. The visit starts with a detailed history of prior nasal procedures, review of operative reports when available, and discussion of any implants or grafts previously used. Knowing what was performed informs expectations about remaining septal reserve, scar planes, and likely donor‑site needs. When records are unavailable, a thorough physical exam and intraoperative contingencies guide the reconstructive plan.
Clinic examination combines static inspection with dynamic airway assessment. External analysis evaluates dorsal contour, tip support, and symmetry. Intranasal inspection assesses septal deviation, mucosal health, turbinate size, and dynamic collapse of the internal or external valve during breathing. Nasal endoscopy (a thin flexible camera) is used selectively to visualize internal anatomy clearly when symptoms suggest complex airway pathology. Standardized photographs document baseline anatomy and support shared decision‑making during follow‑up.
Planning focuses first on restoring a stable framework to permit predictable long‑term shape and function. Dr. Mourad determines whether septal cartilage is available for grafting or whether conchal or costal cartilage will be required, and he explains the tradeoffs for each donor site. He outlines whether an open or closed approach is preferable and whether staging will reduce tension and improve outcomes. Patients receive a written summary of the proposed plan, alternatives, and a timeline for recovery and staged procedures if indicated.
02 · Ideal Candidates
Who benefits from revision rhinoplasty.
A suitable candidate presents with documented anatomic problems after prior surgery and reasonable expectations about achievable change. Indications include persistent dorsal deformity, tip support loss, symptomatic nasal obstruction tied to structural deficits, visible asymmetry, or complications from prior grafts or implants. Ideal candidates are in good general health, have completed initial healing, and can provide prior operative reports or photographs when available. The candidacy decision always follows an in‑person assessment that integrates both form and function.
I
Aesthetic Dissatisfaction
Visible cosmetic concerns that remain or appeared after prior surgery — asymmetry, dorsal irregularities, a pinched or over-rotated tip, pollybeak fullness, or a nose that does not look balanced with the rest of the face.
II
Functional Compromise
Breathing difficulty after prior surgery — nasal obstruction, septal deviation, internal or external nasal valve collapse, turbinate problems, or dynamic sidewall collapse that calls for airway-directed revision.
III
Structural Loss
Depleted cartilage and scar tissue that require staged reconstruction. Candidacy is strengthened by nicotine cessation, medical optimization, and a willingness to follow postoperative care.
From the Patient Gallery
Revision Rhinoplasty Before and After Cases
Documented revision rhinoplasty results from the Manhattan practice — each of these patients had prior nasal surgery elsewhere before being treated by Dr. Mourad. Photographed in standardized studio conditions with written photographic consent on file. Individual results vary with anatomy, scarring, and healing; these cases are representative, not predictive.

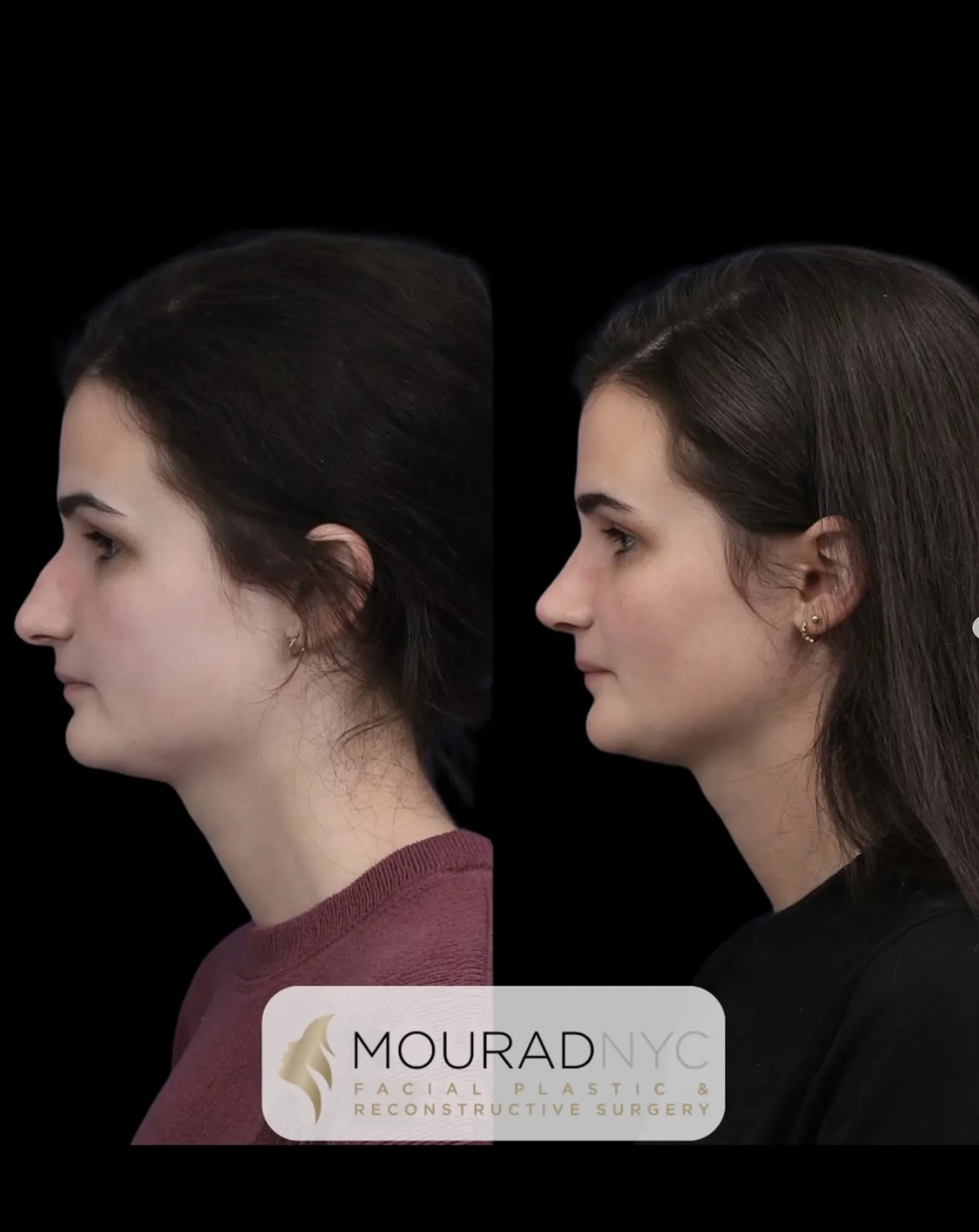
Revision Rhinoplasty · 30s · Female
Revision rhinoplasty for a female patient in her 30s to refine nasal contour and balance the profile following prior nasal surgery. Documented in frontal, oblique, and lateral views before and after surgery; photographed in standardized studio conditions with written consent on file.
Revision Rhinoplasty · 30s · Male

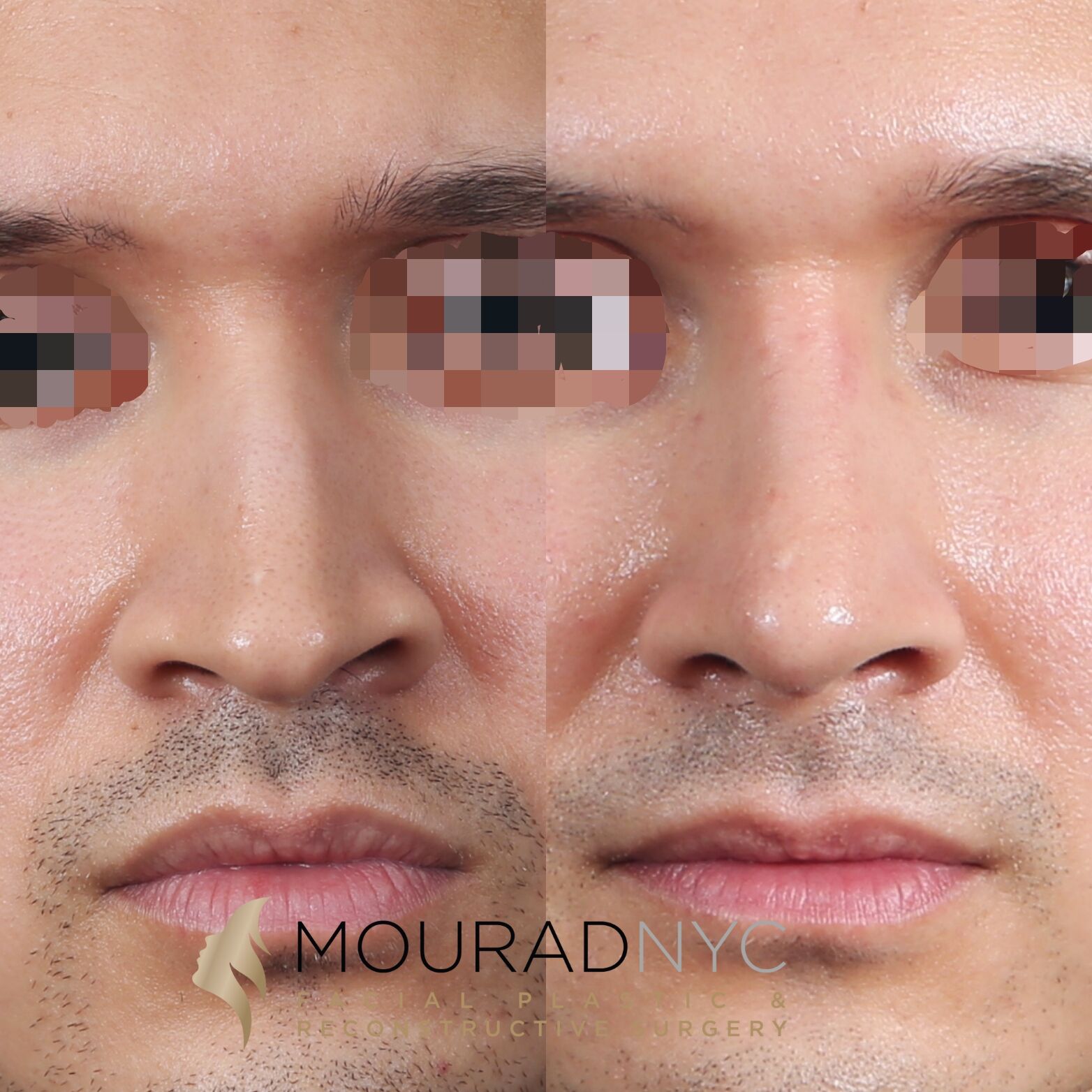
Revision Rhinoplasty · 20s · Female

Revision Rhinoplasty · 30s · Female
Pre and post-operative comparison · Photographed in standardized studio conditions · Written consent on file
If this describes you, the next step is a quiet, unhurried conversation — not a sales call.
An Honest Note
When revision rhinoplasty may not be right for now.
Most revision rhinoplasty should not be performed within twelve months of the prior surgery. The tissues must fully soften and the final settled shape must be visible before re-operating.
Patients whose dissatisfaction is rooted in body-image concerns rather than anatomic findings benefit from a longer, more thoughtful evaluation — sometimes including psychological support — before any further surgery.
Revision in patients with extremely thin skin and depleted cartilage carries elevated risk; the conversation about realistic outcomes is especially important.
Patients seeking dramatic transformation through revision are usually better served by a deliberate, conservative single-stage refinement rather than another aggressive operation.
03 · Approaches
Six paths through a difficult problem.
Revision rhinoplasty is rarely a single technique. The right plan combines several of these elements based on what the prior surgery did and what the tissues will now tolerate.
1 of 6 · Cartilage Graft Revision
Compare your options
Surgery for a blocked nose, side by side
Different structures cause nasal obstruction, and each has a different operation. Select any two options to compare them directly, or open the full table below. The right choice is determined on examination.
What it addresses
Septoplasty: A deviated septum — the wall between the nostrils.
Turbinate Reduction: Enlarged inferior turbinates reducing airway space.
Changes appearance?
Septoplasty: No — purely functional.
Turbinate Reduction: No — internal only.
Incisions
Septoplasty: Hidden, inside the nostril. No external scar.
Turbinate Reduction: Inside the nose, tissue-preserving.
Typical anesthesia
Septoplasty: General or sedation, individualized.
Turbinate Reduction: Often combined with another nasal procedure.
General downtime
Septoplasty: Most desk work resumes within a few days.
Turbinate Reduction: Minimal; frequently done alongside septoplasty.
Insurance
Septoplasty: May be submitted for insurance review when medically necessary and when the patient's plan includes applicable out-of-network benefits.
Turbinate Reduction: May be submitted for insurance review when medically necessary and when the patient's plan includes applicable out-of-network benefits.
View full comparison table
| Attribute | Septoplasty | Turbinate Reduction | Nasal Valve Repair | Septorhinoplasty |
|---|---|---|---|---|
| What it addresses | A deviated septum — the wall between the nostrils. | Enlarged inferior turbinates reducing airway space. | Collapse or narrowing of the nasal valve (sidewall). | The septum and the external shape, together. |
| Changes appearance? | No — purely functional. | No — internal only. | Usually not; focus is structural support. | Yes — functional and cosmetic in one operation. |
| Incisions | Hidden, inside the nostril. No external scar. | Inside the nose, tissue-preserving. | Approach depends on the technique used. | Endonasal or a small columellar incision. |
| Typical anesthesia | General or sedation, individualized. | Often combined with another nasal procedure. | General or sedation, individualized. | General anesthesia, individualized. |
| General downtime | Most desk work resumes within a few days. | Minimal; frequently done alongside septoplasty. | Varies with the technique; discussed at consultation. | A splint for about a week; bruising settles over weeks. |
| Insurance | May be submitted for insurance review when medically necessary and when the patient's plan includes applicable out-of-network benefits. | May be submitted for insurance review when medically necessary and when the patient's plan includes applicable out-of-network benefits. | May be submitted for insurance review when medically necessary and when the patient's plan includes applicable out-of-network benefits. | The functional portion may be submitted for insurance review when medically necessary and when the plan includes out-of-network benefits; the cosmetic portion is self-pay. |
General information only. Anesthesia, downtime, and insurance vary by patient and plan and are determined individually at consultation.
04 · Technique
Costal cartilage vs septal & auricular grafts.
Revision work almost always requires cartilage grafting to rebuild what the prior surgery removed or weakened. The donor site depends on how much structural material is needed and what remains available.
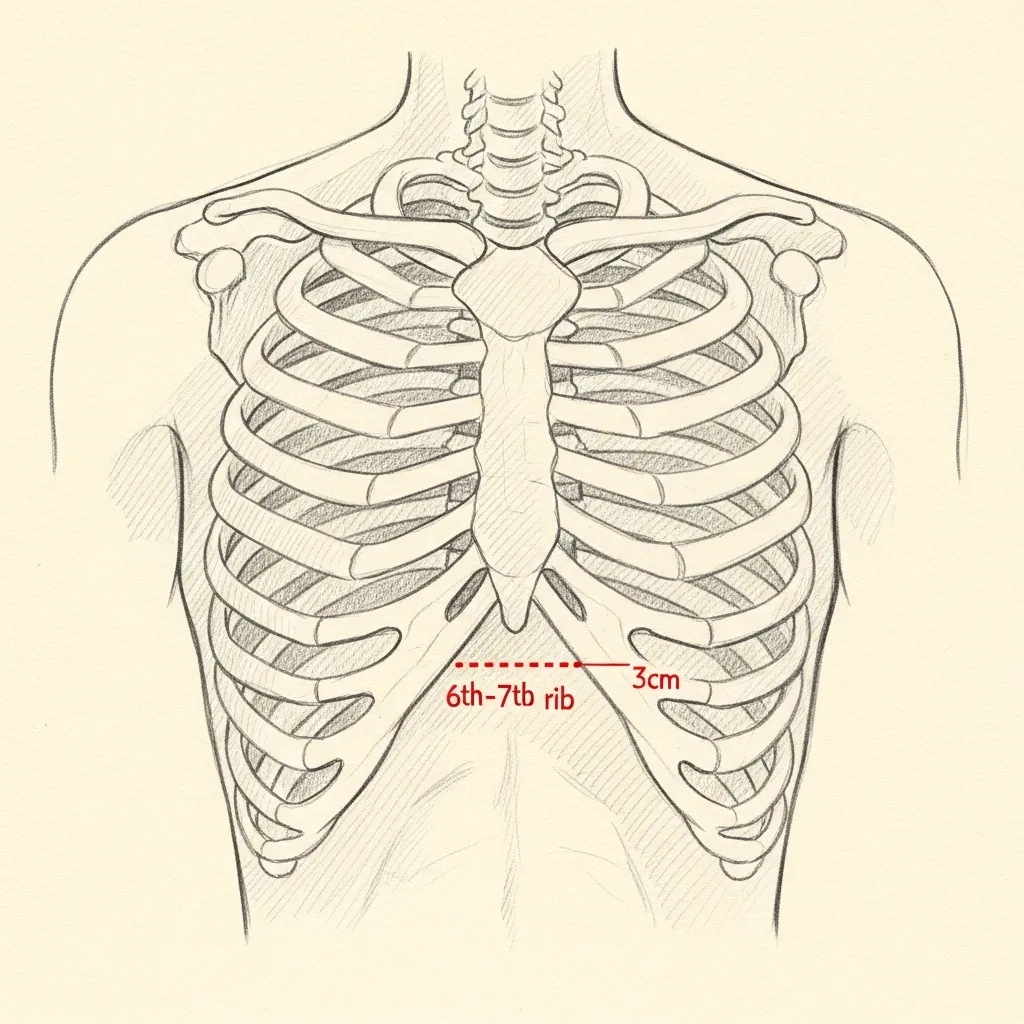
Costal
Rib cartilage for major reconstruction
Costal, or rib, cartilage is often preferred for major revision reconstruction because it can provide abundant, strong graft material when septal and auricular cartilage are depleted.
Harvest is performed through a small hidden incision in the natural inframammary crease. Donor-site discomfort, scarring, and other risks are reviewed during consultation, and pain control is individualized.
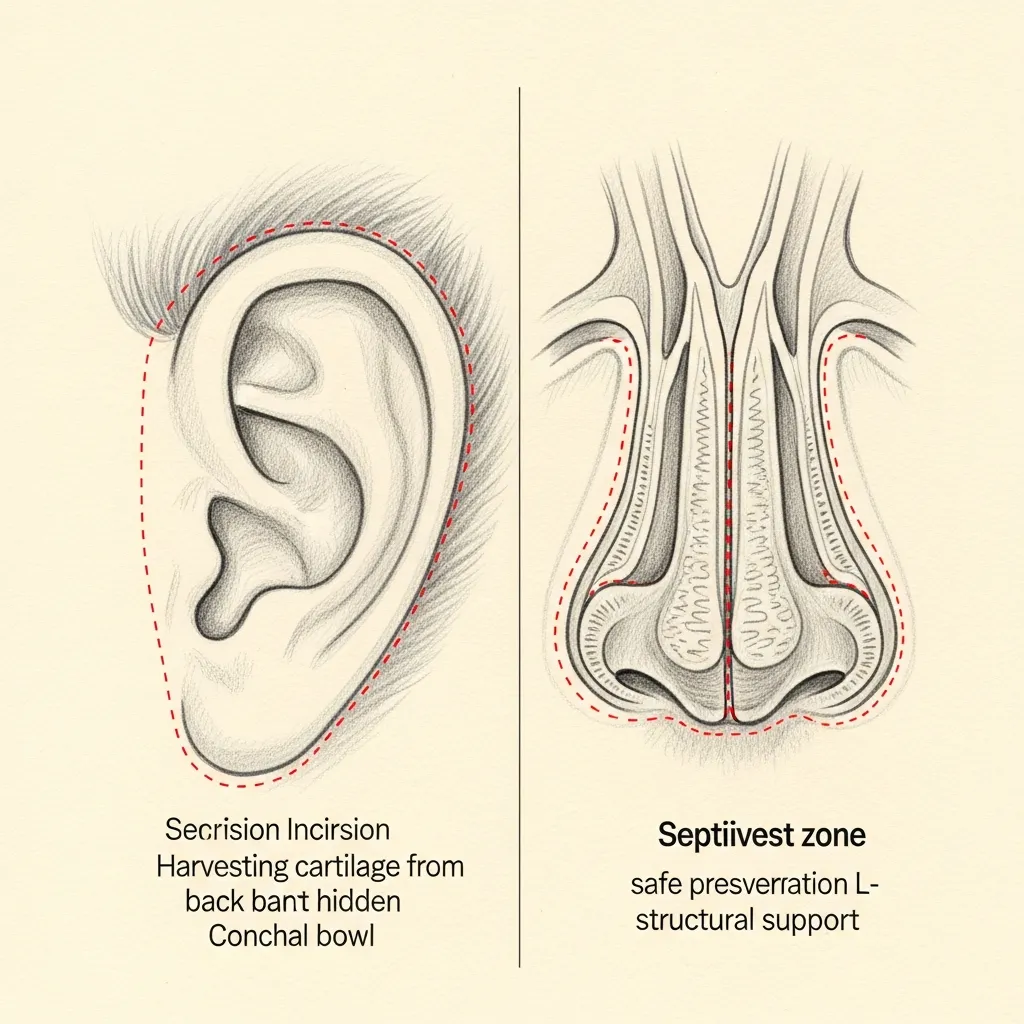
Septal & Ear
Local cartilage when supply allows
Residual septal cartilage is the first-line graft source when sufficient material remains and an L-strut can be safely preserved.
Auricular (conchal) cartilage from behind the ear provides curved, resilient graft material well-suited to lateral wall and lobular reconstruction. The harvest site is hidden in the postauricular crease.
Illustrative diagrams. Graft source is selected case-by-case based on remaining anatomy, structural need, and patient preference.
Graft Sources
Cartilage graft comparison
Revision work almost always requires cartilage grafting to rebuild what prior surgery removed or weakened. The donor source depends on how much structural material is needed and what remains available.
| Best use | Advantages | Limitations & risks | |
|---|---|---|---|
| Remaining septal cartilage | Small to moderate support when available | Same operative field, straight, useful for spreader and smaller structural grafts | Often depleted after prior septoplasty or rhinoplasty; may not provide enough volume for major reconstruction |
| Ear cartilage | Alar support, contour grafts, curved support needs | Autologous tissue, useful curvature, no chest incision | Softer and less rigid than rib; limited quantity; donor-site scar and tenderness possible |
| Autologous rib cartilage | Major structural reconstruction, saddle nose, depleted septum, severe valve collapse | Strong, abundant, durable, the patient's own tissue | Chest incision, donor-site pain or scar, rare pneumothorax, warping risk, longer operation |
| Cadaveric rib cartilage | Selected structural grafting when avoiding a donor-site harvest | Avoids chest incision and rib-harvest pain; available volume | Not the patient's own tissue; variable behavior; possible resorption, warping, infection, displacement, or less predictable long-term support |
| Synthetic / alloplastic implant | Historically used in some nasal augmentation cases | No cartilage harvest; immediate shape support | Higher concerns for infection, extrusion, exposure, skin thinning, migration, and long-term complications in many revision contexts |
Graft source is selected case-by-case based on remaining anatomy, structural need, donor-site considerations, and patient preference.
Begin the conversation
A revision consultation is a careful, honest evaluation — not a sales conversation.
Revision Rhinoplasty Pricing Overview
Surgeon-Specific Planning Estimate
Revision Rhinoplasty With Dr. Mourad
Commonly quoted from approximately $25,000
Many cases are approximately $35,000
Estimated surgeon's fee*
Selected limited revisions may be lower after evaluation. Multiply operated, graft-intensive, implant-related, airway-reconstruction, or structurally complex cases may be higher.
* Eligible medically necessary functional components may be submitted to insurance. Cosmetic portions remain self-pay. Coverage, authorization, deductibles, coinsurance, allowed amounts, and patient responsibility vary by plan and are not guaranteed.
Final pricing follows clinical evaluation.
Revision pricing varies more widely because every prior operation changes the anatomy, scar tissue, cartilage supply, skin envelope, and degree of structural support. Factors that may increase the scope and cost include multiple prior open rhinoplasty procedures, dense scar tissue, depleted septal cartilage, nasal valve collapse, implant or graft removal, rib or ear cartilage grafting, septal perforation, major airway reconstruction, prolonged operative time, and more extensive postoperative care.
MouradNYC is an out-of-network practice. Eligible medically necessary functional components may be submitted to insurance when the patient's plan includes applicable out-of-network benefits and plan requirements are met. Cosmetic portions remain self-pay. Coverage, authorization, deductibles, coinsurance, allowed amounts, and patient responsibility vary by plan and are not guaranteed. Verification and authorization do not guarantee payment.
Published pricing is intended to provide a realistic planning estimate, not a binding quote. Every operation is individualized. Final pricing is determined only after clinical evaluation and may change if the operative plan changes.
The figures shown represent the estimated surgeon's fee. Facility, anesthesia, laboratory testing, medical clearance, imaging, prescriptions, and other services may be billed separately.
Pricing last reviewed: June 2026.
05 · In Dr. Mourad's Words
Revision rhinoplasty videos.
Short educational films and patient perspectives from the Manhattan practice.
Rhinoplasty with Dr. Mourad
An overview of Dr. Mourad's approach to rhinoplasty in his Manhattan practice.
Patient Perspective
A patient discusses her revision experience before, during, and after surgery.
Inside the Consultation
How Dr. Mourad evaluates revision anatomy, prior records, and surgical candidacy.
06 · Recovery
What revision healing actually looks like.
Stage 01
First 24 Hours
The first day centers on rest and protection of the repair. Expect a splint or cast on the bridge, support inside the nose, congestion, and some oozing managed with gentle head elevation. Pain is usually moderate and controlled with prescribed medication. Bending, lifting, and any straining that raises pressure in the nose are avoided.
Stage 02
Week 1
Through the first week swelling and bruising around the eyes and nose are most noticeable and then begin to settle. The external splint and any internal splints or sutures are typically removed near the end of this week. Many patients feel presentable enough for desk-based work once the splint is off, while strenuous activity remains off-limits.
Stage 03
Weeks 2 – 4
Over weeks two to four the obvious bruising resolves and the early shape of the rebuilt nose emerges, though the tip stays firm and slightly swollen. Light exercise is reintroduced gradually on the surgeon's guidance. Because revision tissue is scarred and less predictable, swelling in this phase can fluctuate more than after a first-time rhinoplasty.
Stage 04
Months 1 – 18
Refinement continues longer than most patients expect. Deep tip swelling in a revision nose can take roughly twelve to eighteen months to fully resolve, and the final contour is assessed at the end of that window. Grafted cartilage settles, the skin redrapes, and small asymmetries common in early healing typically continue to improve over this period.
Have a specific question?
Send a brief note describing your anatomy or concerns — the office will route it directly to Dr. Mourad for review.
Twelve to Eighteen Months
Long-term healing.
Outcomes after revision rhinoplasty evolve across predictable phases that reflect healing, graft integration, and scar remodeling rather than a single endpoint. The early phase is characterized by edema, bruising, and firm tissues that obscure fine contours. The intermediate phase entails graft settling, soft-tissue relaxation, and improving nasal symmetry as inflammation resolves. The late phase, typically approaching twelve months, reveals more stable tip definition and dorsal refinement, though subtle changes may continue for longer in complex reconstructions. Because revision cases usually involve added structural work, the surgeon anticipates gradual maturation and plans follow-up accordingly.
Functional improvements in airway patency follow a similar multi-stage course and depend on both mechanical repair and mucosal recovery. Septal reconstruction, turbinate reduction, and valve support procedures reduce structural blocks to airflow, but mucosal swelling and scar contracture influence subjective breathing for months. Objective assessment with nasal endoscopy, validated patient-reported outcome measures, or airflow testing at follow-up visits helps track progress in both subjective and measurable terms. Successful functional outcomes therefore rely on combined surgical mechanics and postoperative medical care tailored to mucosal health.

Safety & Consent
Risks, safety, and informed consent.
Revision rhinoplasty carries specific risks that differ from primary procedures because scarred tissue and prior grafting change the operative landscape. Bleeding and hematoma formation remain early risks and can compromise grafts or require urgent drainage in the operating room. Septal hematoma (a collection between nasal septum layers) produces worsening pain and obstruction and requires prompt drainage to avoid cartilage loss. Mitigation includes meticulous intraoperative hemostasis, perioperative blood-pressure control, and early postoperative monitoring for expanding nasal fullness or new drainage that suggests a hematoma.
Infection is a recognized complication that may present with fever, increasing pain, erythema, and purulent drainage from incision or donor sites. Alloplastic implants have a higher risk of late exposure and infection compared with autologous grafts, and implant-related infections sometimes mandate removal. To reduce infectious risk we apply strict sterile technique, judicious antibiotic use when indicated, and selection of autologous tissue when feasible. Early identification of infection allows office-based irrigation and targeted antibiotics or timely operative washout when necessary to protect structural grafts.

Before You Arrive
Your revision consultation, prepared.
Bring operative reports from any prior nasal surgery if available.
Bring pre-operative photographs from your prior surgery if available.
Note any breathing changes since your prior surgery — when, how severe.
List all medications, supplements, and blood-thinning agents.
Allow 75 minutes; revision consultations are deliberately longer.
No decisions are made at the first visit — that is by design.
In Their Words
From patients of the practice.
Revision surgery made me nervous because I had already been through one rhinoplasty elsewhere. This time felt very different. Everything was explained clearly, and the result looks much more balanced.
I had breathing issues and cosmetic concerns after my first surgery years ago. My revision was not rushed, and I appreciated the honesty about what could and couldn't be fixed. My nose looks softer and functions better.
I wanted a revision but was scared of making things worse. The plan was conservative, and that gave me confidence. I finally feel like my nose fits my face.
I flew in for revision rhinoplasty after several consultations that didn't feel right. This was the first time I felt someone really understood the problem. The improvement has been a huge relief.
Individual experiences. Results and recovery vary by patient. Testimonials shared with written consent.
Patient Reviews
Revision Rhinoplasty Patient Experiences
Selected public patient reviews. Individual experiences vary.
“After a really difficult first surgery, I was hesitant about revision rhinoplasty, until I met Dr. Mourad. He was incredibly warm and attentive from the start…”
Real patient experiences
Selected public reviews from patients of the practice.
Your privacy matters
We never share personal health information.
Board-certified expertise
Dual board-certified facial plastic and reconstructive surgeon.
Individual results vary. Reviews reflect individual experiences and are not a guarantee of outcome.
At a Glance
Revision rhinoplasty fact snapshot.
- Treats
- Structural collapse, breathing obstruction, asymmetry, over-resection, tip deformity, and bridge irregularities after a prior rhinoplasty.
- Does not treat
- Concerns unrelated to the prior surgery, or expectations of an entirely different nose — revision works within the limits of the remaining tissue.
- Evaluation
- In-person examination of the internal and external nose, review of prior operative records when available, and sometimes imaging.
- Related conditions
- Nasal valve collapse, deviated septum, and post-surgical airway obstruction.
- Possible combined procedures
- Septoplasty, nasal valve repair, and cartilage grafting from the septum, ear, or rib.
- Recovery summary
- Most patients return to desk work in one to two weeks; swelling resolves gradually over a year or more, often slower than after a primary rhinoplasty.
- Insurance / functional distinction
- The functional airway component may be submitted for insurance review — coverage is never guaranteed; cosmetic revision is self-pay. This out-of-network practice provides documentation for reimbursement.
- When to seek evaluation
- Once healing has stabilized — typically around a year after the prior surgery — or sooner for significant breathing obstruction.
Find your starting point
Which nasal breathing path fits your situation?
Answer three short questions to see which page explains the evaluation most relevant to you. This is educational orientation, not a diagnosis — a clinical examination is how the cause of nasal obstruction is actually determined.
Select an option for each question to see which page fits your situation.
This guide is general educational information, not medical advice or a diagnosis. Only an in-person examination can determine the cause of nasal obstruction and the appropriate treatment.
See all pathways
A combined revision evaluation likely fits
When both breathing and appearance are concerns after previous surgery, the anatomy is already altered and rebuilding structural support is often part of the plan. A revision evaluation looks at what the prior operation changed before anything is recommended.
A revision rhinoplasty conversation likely fits
Changing the appearance of a nose that has already had surgery is a different undertaking from a first operation, because scar tissue and prior changes shape what is possible. A revision evaluation is the right starting point.
A deviated-septum evaluation likely fits
Persistent, constant blockage that does not resolve with sprays or allergy treatment is often related to a deviated septum. Septoplasty is the functional operation that straightens the septum. If you have had prior nasal surgery, revision considerations also apply.
A nasal valve evaluation likely fits
When the side of the nose draws inward on hard inspiration, the nasal valve — the narrowest part of the airway — may be the contributor rather than the septum alone. This is assessed directly on examination.
A turbinate and sinus evaluation likely fits
Congestion that fluctuates with colds, allergies, or facial pressure often involves swollen turbinates or the sinuses rather than the septum by itself. The evaluation looks at the whole airway before any procedure is considered.
A septorhinoplasty conversation likely fits
When breathing and appearance are both concerns, they can often be addressed together in a single planned operation — straightening the septum while refining the external shape — so there is one recovery rather than two.
A rhinoplasty conversation likely fits
When the concern is the shape of the nose, rhinoplasty is the operation that refines it. A consultation focuses on your goals and whether the underlying anatomy supports them.
A revision evaluation likely fits
After previous nasal surgery, a fresh structural evaluation is the right starting point because the anatomy has already been changed once.
Start with a functional nasal evaluation
Your answers point to more than one possible contributor, which is common. A functional nasal examination is how the cause is identified before any treatment is considered.
Why patients trust this practice
Care led by a double board-certified specialist
Double board certified
American Board of Facial Plastic & Reconstructive Surgery and American Board of Otolaryngology — Head & Neck Surgery.
AAFPRS Fellowship Director
Trains fellows through the American Academy of Facial Plastic and Reconstructive Surgery.
Published author
Contributions to the academic literature of facial plastic surgery.
Face, nose & sinus focus
A practice concentrated above the clavicles, including complex revision evaluations.
Frequently Asked
Revision Rhinoplasty NYC FAQs
Revision rhinoplasty cost in NYC is highly individualized because the surgeon may be working with scar tissue, altered anatomy, depleted cartilage, breathing obstruction, or the need for grafting. There is no flat price; the fee reflects the surgical complexity, anesthesia, and facility costs for your specific case. A personalized estimate is provided after an in‑person consultation.
Cosmetic refinements are generally self‑pay. If part of the revision corrects a documented functional problem such as nasal obstruction, valve collapse, or septal deviation, insurance may apply to the functional portion. Coverage depends on your plan, medical necessity, and documentation. Our office can help you understand what records may be needed and what out‑of‑pocket costs may apply.
Most revision rhinoplasty is best deferred until at least twelve months after the prior surgery, so soft tissue swelling resolves and the final settled shape is visible before re‑operating. Earlier intervention is sometimes necessary in specific situations such as infection or implant exposure, and is often staged. Timing is individualized at the consultation.
Revision is more complex because the normal anatomy has already been altered. Scar tissue distorts the tissue planes, the original cartilage may be depleted, the skin envelope can be thinned, and structural support is often weakened by prior reduction. These factors make exposure, grafting, and reshaping more demanding than in a first‑time rhinoplasty.
Not always. When sufficient material remains, septal cartilage is the first‑line graft source, and ear (conchal) cartilage is useful for curved contour grafts. Costal (rib) cartilage is reserved for major rebuilding when septal and ear sources are depleted or significant structural support must be restored. The graft source is selected case‑by‑case based on what the anatomy requires.
Revision can improve breathing when a structural cause is identified and addressed, such as septal deficiency, internal valve narrowing, or valve collapse. Techniques may include septal reconstruction and spreader or batten grafts, sometimes combined with turbinate management. The degree of improvement depends on tissue quality and prior surgery, and is assessed with examination and endoscopy at consultation.
Common concerns include an over‑rotated or pinched tip, asymmetry, a saddle deformity from over‑resection, a residual hump, pollybeak fullness, and dorsal lines that are no longer straight. Functional problems such as valve collapse or a septal perforation sustained during prior surgery can also be addressed. Each issue is mapped and prioritized during planning.
Primary rhinoplasty is a first nasal operation on tissue that has not been previously altered. Revision rhinoplasty is performed on a nose that has already had surgery, where scar tissue, depleted cartilage, and weakened support change the plan. If you have never had nasal surgery, primary rhinoplasty is the right starting point rather than this page.
Secondary rhinoplasty is another term for revision rhinoplasty — nasal surgery performed on a nose that has already had one or more previous operations. It is the same type of procedure described on this page, addressing the altered anatomy, scar tissue, and depleted cartilage left behind by prior surgery.
The open approach is frequently chosen for revision because it gives direct exposure for scar release, accurate graft placement, and structural rebuilding. A closed approach can be appropriate for limited, well‑defined adjustments. There is no single right answer; the approach is selected based on scar burden, grafting needs, and airway goals, and the reasoning is explained during planning.
Early bruising and most visible swelling generally settle over the first two to three weeks, similar to primary surgery, and the splint is typically removed near the end of the first week. Because revision tissue is scarred, deeper swelling can take longer to resolve. Light activity is reintroduced gradually on your surgeon's guidance.
Refinement in a revision nose continues longer than many patients expect. Deep tip swelling can take roughly twelve to eighteen months to fully resolve, and the final contour is assessed at the end of that window as grafted cartilage settles and the skin redrapes. Individual healing varies, and small early asymmetries commonly continue to improve over this period.
Bring operative reports from any prior nasal surgery and pre‑operative photographs if you have them, along with a list of your medications, supplements, and any blood‑thinning agents. Note any breathing changes since your prior surgery — when they began and how severe they are. These records make the evaluation more accurate; no surgical decisions are made at the first visit.
Clinical references
This page draws on published clinical practice guidelines and public-health references. These sources inform general patient education and do not replace an individual evaluation with Dr. Mourad.
- 01Ishii LE, et al. Clinical Practice Guideline: Improving Nasal Form and Function after Rhinoplasty. Otolaryngology–Head and Neck Surgery. 2017;156(2 suppl):S1–S30. AAO-HNSF guideline
- 02U.S. National Library of Medicine (MedlinePlus). Nose Injuries and Disorders. MedlinePlus
- 03Rhinoplasty. StatPearls. Treasure Island (FL): StatPearls Publishing; NCBI Bookshelf. StatPearls (NCBI Bookshelf)
- 04Reconstructive rhinoplasty: operative revision of patients with previous autologous costal cartilage grafts. U.S. National Library of Medicine, PubMed. PubMed
Related Nasal Surgery
Explore related procedures and resources.
Revision is the right path only for patients with prior nasal surgery. If your situation is different, these pages may be a better starting point.
Primary rhinoplasty in NYC
For patients who have never had nasal surgery and are considering a first rhinoplasty.
Read moreSeptoplasty for a deviated septum
When the primary concern is breathing through a deviated septum rather than appearance.
Read moreNasal valve collapse treatment
Repair of internal or external valve collapse that restricts the nasal airway.
Read moreSeptal perforation repair
Closure of a hole in the septum, sometimes sustained during prior nasal surgery.
Read moreBroken nose repair
Evaluation and repair after recent nasal trauma or a post-traumatic deformity.
Read moreRevision rhinoplasty cost in NYC
What affects revision surgery fees — surgeon, facility, anesthesia, rib or ear cartilage grafting, and insurance.
Read moreCost, financing & insurance
How surgical fees, financing, and insurance for functional repair are approached.
Read moreThe Most Important Step
Your revision consultation.
The appropriate next step is an in-person consultation where prior operative reports, photographs, and imaging are reviewed to shape an individualized plan. Bring all prior surgical records, implant documentation if available, and a clear chronology of functional and cosmetic symptoms to the visit. Expect the consultation to include an external exam and office nasal endoscopy (a flexible scope examination) to assess mucosal health, septal integrity, and valve competence. We will discuss candidacy, whether septal cartilage remains available, the potential need for auricular or costal cartilage, and whether a staged reconstruction is safer for durable results.