Double Board Certified · In-Office Nasal Procedure
Vivaer Nasal Airway Remodeling — an in-office option for the right patient.
Vivaer is an in-office, non-surgical procedure that uses low-temperature radiofrequency to remodel the internal nasal valve. For the right patient —…
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"Vivaer is right for some patients and wrong for many. The job at consultation is to know the difference."
A Note from Dr. Mourad
"Vivaer is an in-office, non-surgical procedure that uses low-temperature radiofrequency to remodel the internal nasal valve. For the right patient — mild-to-moderate valve collapse without major septal deviation — it is a reasonable alternative to surgery."
— Dr. Moustafa Mourad, MD
Overview
What is VivAer nasal airway remodeling?
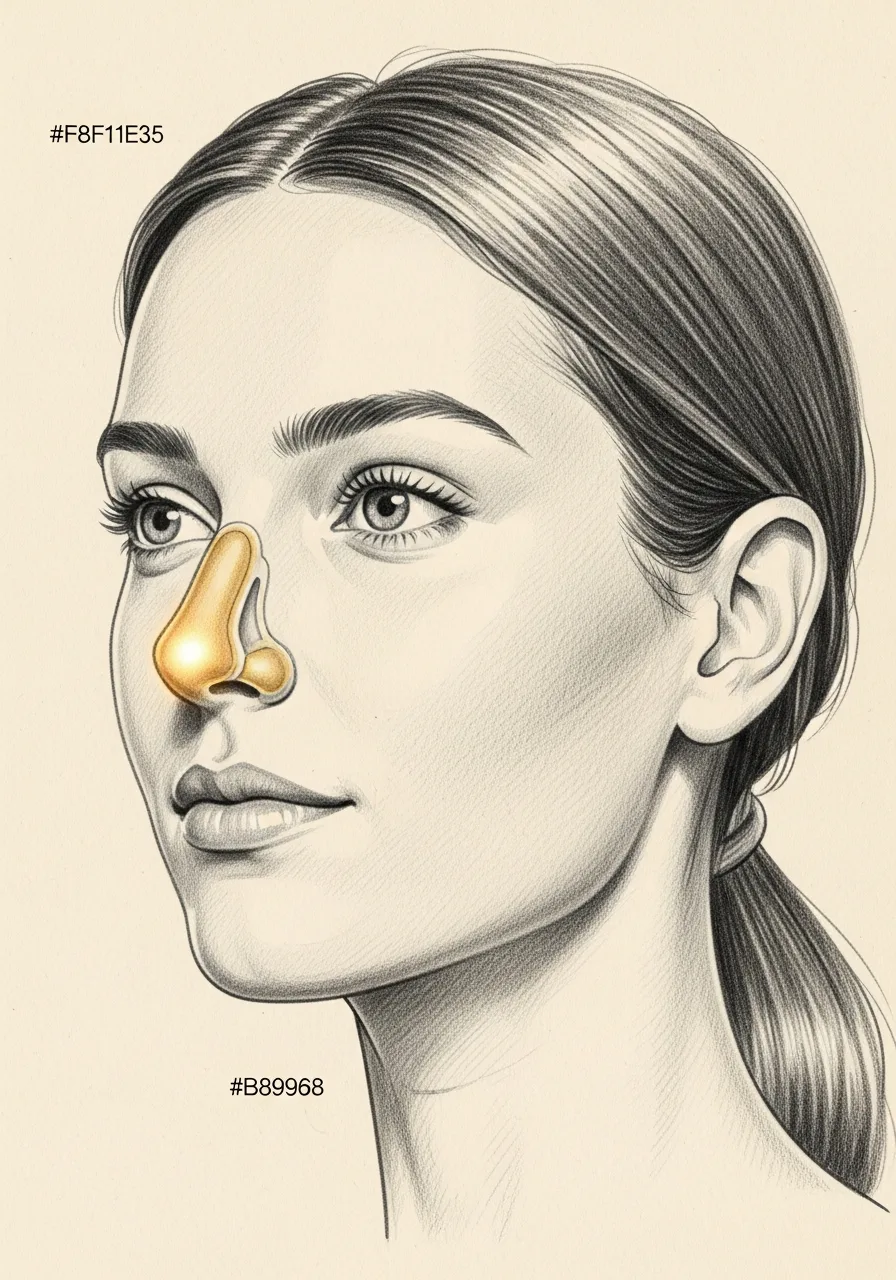
VivAer is an in-office, non-surgical procedure that uses controlled, low-temperature radiofrequency energy to remodel the soft tissue of the internal nasal valve — the narrowest part of the nasal airway. The treatment is delivered through the nostrils under local anesthesia, takes roughly fifteen to twenty minutes, and requires no incisions.
It is considered for patients with nasal obstruction caused by dynamic or static narrowing of the internal nasal valve, particularly when the obstruction is not primarily due to a deviated septum, polyps, or large turbinates. Candidacy is determined by examination, including a manual lateralization (Cottle) test.
VivAer is not a substitute for septoplasty, turbinate reduction, or functional rhinoplasty when those problems are the main driver of obstruction. Used in the right patient and as part of an accurate diagnosis, it is a useful office-based option that avoids the operating room.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
01 · Why Dr. Mourad
Diagnosis first, then a plan that fits.
Dr. Mourad evaluates Vivaer candidacy candidly — the procedure is not a substitute for septoplasty or for structural valve reconstruction when those are the right answer.
When Vivaer is appropriate, it is performed in-office under local anesthesia with minimal recovery.
Patients are counseled honestly about expected duration of improvement and the option to proceed to surgery if needed.
02 · Ideal Candidates
Who benefits most from this operation.
Candidacy is determined together at consultation. The most satisfied patients share three things in common.
I
Mild-to-Moderate Valve Collapse
Patients whose primary obstruction is at the internal nasal valve, without significant septal deviation or turbinate hypertrophy.
II
Recovery-Constrained Patients
Patients who cannot accommodate the recovery from a surgical operation but want meaningful airway improvement.
III
Diagnostic Trial
In selected cases, an in-office trial of valve treatment helps confirm that the valve is the primary site of obstruction before any surgical decision.
From the Patient Gallery
A representative rhinoplasty result.
A female patient in her 20s, documented in standardized studio conditions before and after surgery. Written photographic consent on file. Results vary by patient; this case is representative, not predictive.




Pre and post-operative comparison · Written consent on file
If this describes you, the next step is a quiet, unhurried conversation — not a sales call.
An Honest Note
When this operation may not be right for you.
Patients with significant septal deviation should consider septoplasty as the primary intervention; Vivaer alone will not address structural deviation.
Patients with significant turbinate hypertrophy benefit more from turbinate reduction.
Patients with severe inspiratory valve collapse usually require structural cartilage grafting for durable improvement.
Patients seeking a permanent surgical solution should consider rhinoplasty-based valve reconstruction.
03 · Approaches
Three paths to a better airway.
Vivaer is one option in a broader toolkit. The right choice depends on whether the obstruction is functional, structural, or a combination — and on how much downtime the patient can accept.
1 of 3 · In-Office Vivaer Procedure
04 · Technique
Vivaer vs surgical valve reconstruction.
The same anatomic problem can be approached in-office or in the operating room. The right choice depends on the severity of collapse and what the patient is trying to accomplish.
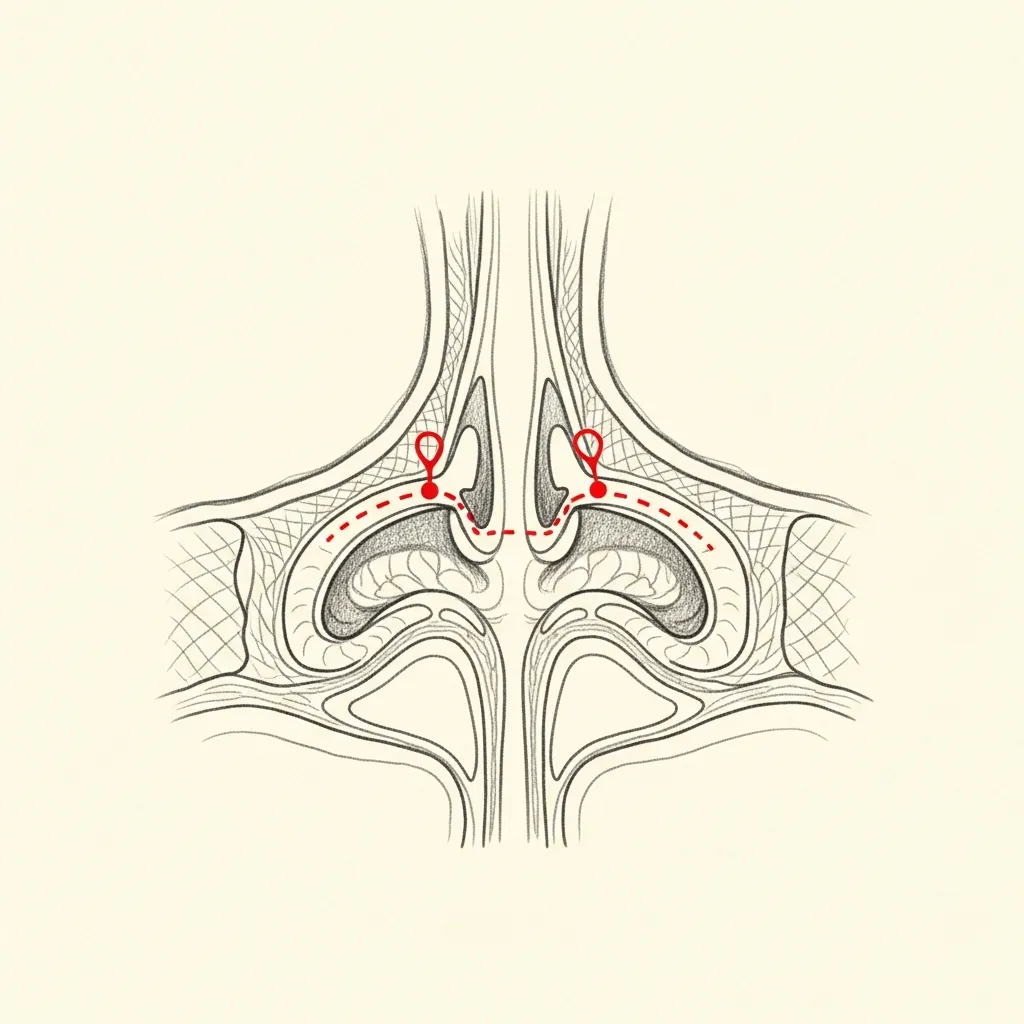
Vivaer
In-office radiofrequency remodeling
Low-temperature radiofrequency energy is applied to specific points along the upper lateral cartilage and septum, causing controlled tissue remodeling that stiffens and reshapes the internal valve.
The procedure takes about 30 minutes in the office. Most patients return to normal activity the same or next day.
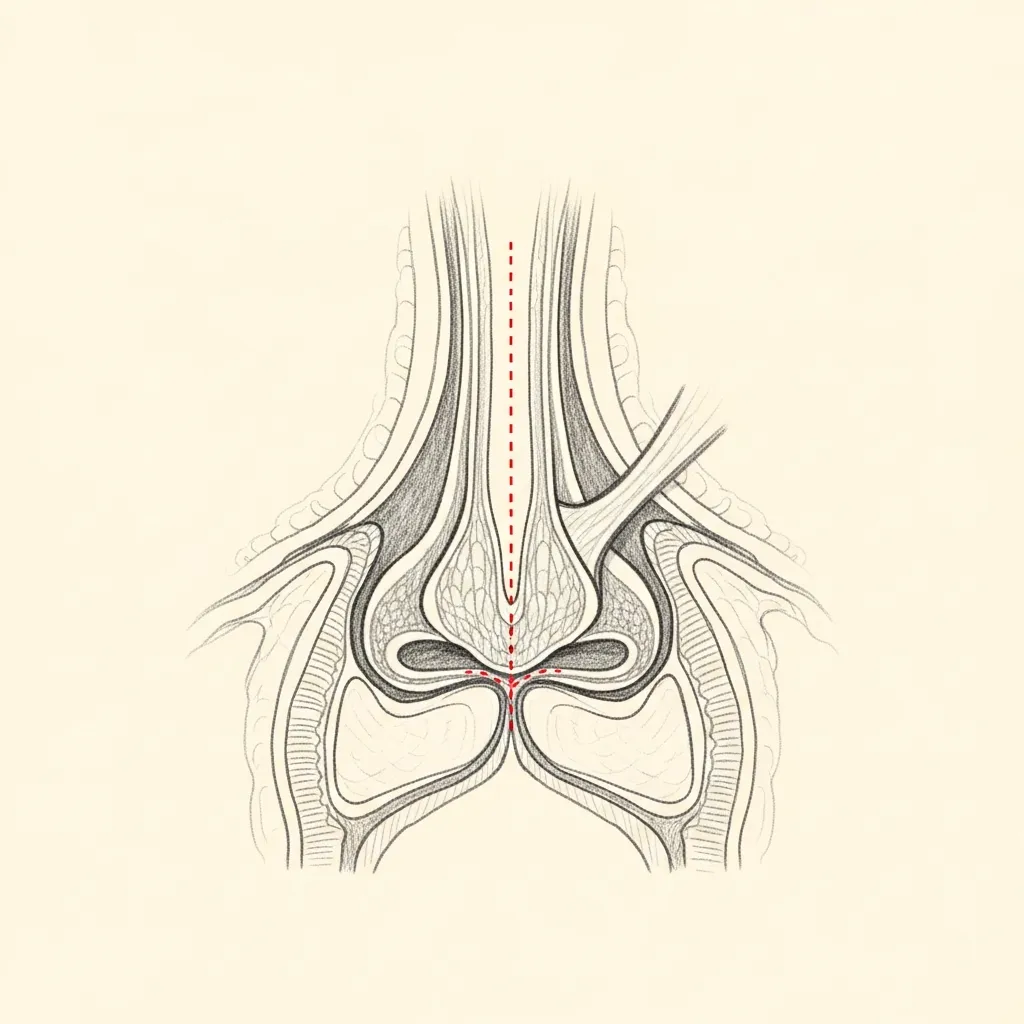
Surgical
Spreader grafts for durable structural support
When valve collapse is more severe — or when other rhinoplasty work is being performed — spreader grafts provide definitive structural support to the internal valve.
This is a longer-recovery operation but the structural change is permanent and durable.
Illustrative diagrams. The right choice is determined by the severity of collapse and the patient's goals.
Begin the conversation
A careful, honest evaluation is the right first step.
Cost, Financing & Insurance
Vivaer Nasal Airway Remodeling Cost, Financing & Insurance in NYC
The cost of Vivaer nasal airway remodeling depends on the anatomy being treated, the extent of airway obstruction, and whether the treatment is performed alone or as part of a broader nasal airway plan. Vivaer is typically performed in office under local anesthesia.
Because Vivaer treats nasal airway obstruction, it may be covered by insurance when it is medically necessary. Coverage often depends on symptoms, examination findings, prior treatment, and the patient’s insurance plan. Our office can help review benefits and guide patients through preauthorization when appropriate.
What May Affect Cost
- Extent of airway obstruction
- Anatomy being treated
- Whether combined with other nasal treatment
- In-office local anesthesia
- Prior nasal treatment
- Insurance plan requirements
This information is educational and is not a guarantee of pricing, insurance coverage, reimbursement, financing approval, or surgical candidacy. A personalized estimate is provided after consultation. Insurance coverage depends on the patient’s plan, medical necessity, documentation, and carrier requirements. Financing terms are determined by third-party financing providers.
05 · In Dr. Mourad's Words
Educational videos.
Short educational films and patient perspectives from the Manhattan practice.
Dr. Mourad in Practice
An overview of the practice and philosophy.
Patient Perspective
A patient discusses her experience before, during, and after surgery.
Inside the Consultation
How Dr. Mourad evaluates anatomy, goals, and candidacy.
06 · Recovery
What healing actually looks like.
Stage 01
First 24 Hours
Initial recovery focuses on rest, hydration, and following all post-operative instructions exactly. Pain is managed with multi-modal non-narcotic protocols where appropriate.
Stage 02
Week 1
Swelling and bruising peak in the first few days and improve steadily through the first week. Most patients are presentable for casual social activity by the end of week two.
Stage 03
Weeks 2 – 4
Through weeks two to four the early result begins to settle. Light cardio resumes around three weeks; vigorous exertion and contact activities are deferred per the operative plan.
Stage 04
Months 1 – 6
The final refined result emerges progressively over the following months as residual swelling continues to resolve. Follow-up visits are scheduled across the first year.
Have a specific question?
Send a brief note describing your anatomy or concerns — the office will route it directly to Dr. Mourad for review.

Before You Arrive
Your consultation, prepared.
Bring photographs relevant to your concern, when available.
Bring records from any prior surgery, when available.
List current medications, supplements, and blood-thinning agents.
Note any prior anesthesia issues or chronic medical conditions.
Allow 60 minutes for the first consultation.
Bring questions; no decisions are made at the first visit.
Frequently Asked
Patient questions, honestly answered.
VivAer uses a low‑temperature radiofrequency device applied inside the nasal cavity to induce controlled collagen remodeling of tissues at the internal nasal valve. The goal is to stiffen and reshape the valve region to resist collapse during inspiration. This is an office‑based procedure performed under topical and local anesthesia, with no external incisions in most cases. Final determination of suitability requires an in‑person exam including dynamic testing.
Candidates typically have symptomatic, mild‑to‑moderate internal nasal valve narrowing with preserved cartilage architecture and localized soft‑tissue laxity. Patients with severe structural collapse, major external deformity, or unstable septal support are usually better served by formal surgical reconstruction. Prior septoplasty or rhinoplasty does not automatically exclude candidacy; cartilage integrity and dynamic function are the deciding factors. Candidacy is confirmed after nasal endoscopy and dynamic maneuvers in clinic.
VivAer is an office‑based, tissue‑remodeling technique that targets the internal valve soft tissues rather than repositioning or grafting cartilage. Septoplasty corrects a deviated septum and is directed at central structural obstruction, while formal valve reconstruction typically involves cartilage grafting or structural support under general anesthesia. VivAer may be appropriate when valve collapse is primarily soft‑tissue‑mediated and cartilage support is adequate. When cartilage deficiency or major deformity exists, operative repair remains the standard.
The procedure begins with topical and local anesthesia and ends with brief post‑procedure observation. The VivAer wand is introduced into the internal valve region and treated in short applications following a planned pattern. Most treatments are completed within 10–30 minutes depending on bilateral need and extent of treatment. Patients usually leave the office the same day.
Discomfort is generally mild and managed with local anesthetic and oral analgesics as needed. Expect mild swelling, crusting, and congestion for about 3–14 days, with most patients returning to routine activities within 24–72 hours. Strenuous exercise is usually deferred for 1–2 weeks. An in‑person follow‑up is arranged within 1–6 weeks to assess healing and symptom change.
Many patients report subjective improvement within days to a few weeks as swelling settles and collagen remodeling begins. Objective remodeling continues over 6–12 weeks, and clinical durability may last months to years depending on tissue quality and underlying anatomy. VivAer is not guaranteed to permanently correct every case; some patients may require additional treatment or formal surgical repair for durable improvement. Long‑term outcomes vary by individual anatomy and prior surgery.
VivAer is designed to act internally at the valve and does not involve external incisions or deliberate reshaping of nasal framework in most cases. Minor, subtle contour changes are possible but uncommon and typically clinically insignificant. Patients seeking cosmetic change or correction of external deformity should discuss septorhinoplasty or formal structural techniques instead. Any anticipated external effect is reviewed during the consultation.
Common short‑term effects include localized swelling, crusting, mild discomfort, and transient nasal congestion that usually resolve in 3–14 days. Less common risks include prolonged numbness, persistent crusting, or, rarely, localized thermal injury. Significant complications are uncommon with proper technique and office safety measures. All risks are reviewed during the consent process and candidacy requires in‑person evaluation.
VivAer may be staged or performed concurrently with septoplasty or turbinate reduction when multiple contributors to obstruction exist. In many cases, addressing the septum or hypertrophic turbinates simultaneously provides a more comprehensive airway improvement. The decision to combine procedures depends on the anatomy, severity of obstruction, and operative logistics. Dr. Mourad reviews combined options and timing during the consultation.
Insurance coverage for VivAer varies by insurer and the documented medical necessity; some plans require prior authorization while others may not cover office‑based radiofrequency treatments. The practice provides documentation of symptoms and clinical findings to support coverage requests when appropriate. Patients should verify benefits with their insurer and the office can assist with preauthorization and billing questions. Financial counseling is provided prior to scheduling.
The Most Important Step
Your expert consultation.
A careful evaluation by a double board-certified physician is the right first step. The conversation is unhurried, the diagnosis is honest, and the operative plan is built around what your anatomy can sustain and what you actually want.