Double Board Certified · AAFPRS Fellowship Director
Rhinoplasty NYC — Recognized by Modern Luxury for Best Rhinoplasty
Dr. Moustafa Mourad performs rhinoplasty in NYC, including cosmetic rhinoplasty, functional septorhinoplasty, preservation rhinoplasty, and revision rhinoplasty. His approach prioritizes natural facial balance, durable nasal support, and breathing function.
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director

In Consultation
"The goal is enhancement, not transformation."
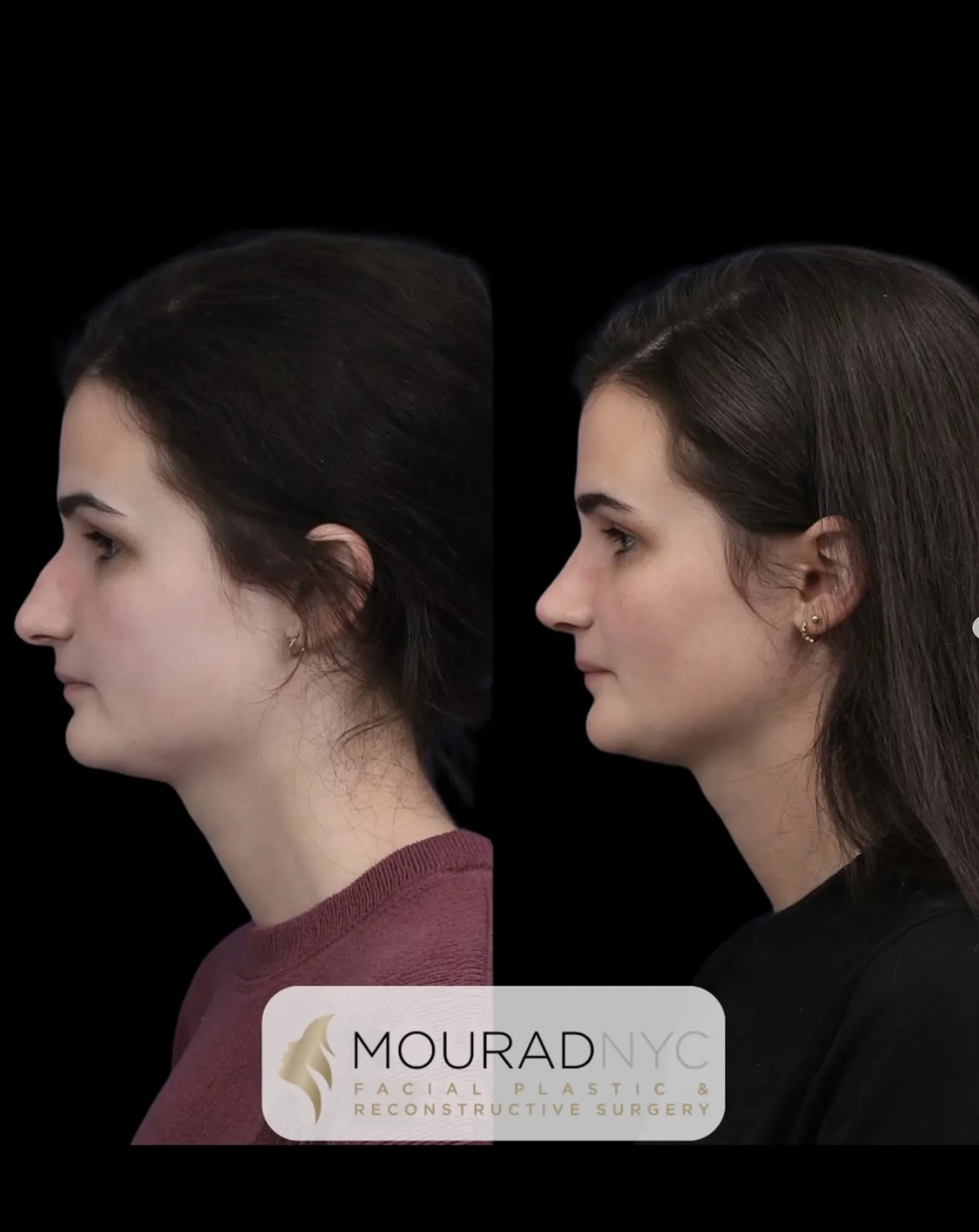
Before & After
Rhinoplasty results from the practice.

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty · 20s · Female

Revision Rhinoplasty · 30s · Male

Ethnic Rhinoplasty · 40s · Male

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty · 40s · Female

Primary Rhinoplasty · 30s · Female

Ethnic Rhinoplasty · 30s · Male

Primary Rhinoplasty + Sinus Surgery · 40s · Female

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty + Sinus Surgery · 20s · Female

Primary Rhinoplasty · 30s · Female

Primary Rhinoplasty · 50s · Male

Primary Rhinoplasty + Sliding Genioplasty · 20s · Male

Revision Rhinoplasty + Sinus Surgery · 30s · Male

Ethnic Rhinoplasty · 20s · Male

Primary Rhinoplasty + Sinus Surgery · 20s · Female

Ethnic Rhinoplasty + Sinus Surgery + Broken Nose Repair · 30s · Female

Revision Rhinoplasty · 20s · Female
Primary Rhinoplasty + Broken Nose Repair · 20s · Female

Revision Rhinoplasty · 30s · Female

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty + Neck Lift · 30s · Female

Revision Rhinoplasty · 30s · Female

Revision Rhinoplasty · 40s · Female

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty · 20s · Male

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty · 20s · Female

Facelift + Neck Lift + Rhinoplasty · 50s · Female

Revision Rhinoplasty · 30s · Female

Primary Rhinoplasty + Broken Nose Repair · 20s · Female

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty · 20s · Female

Primary Rhinoplasty · 20s · Female
Pre and post-operative comparison · Photographed in standardized studio conditions · Written consent on file · Individual results vary
A Note from Dr. Mourad
"In Manhattan, I meet patients filled with apprehension about rhinoplasty. The most common concern — will I look unnatural? What I tell them is simple: preserving your identity is as essential as the refinement itself."
— Dr. Moustafa Mourad, MD, FACS
Key takeaways
- Rhinoplasty reshapes the external nose, improves breathing, or addresses both in one operation.
- Dr. Mourad evaluates the nose as both an aesthetic and a functional structure.
- Functional rhinoplasty can restore the airway, often alongside septoplasty or nasal valve support.
- Native cartilage is preserved and reinforced, with grafts added when more support is needed.
- The aim is a natural nose that fits your face and preserves your identity.
Overview
What is rhinoplasty?
Patients seeking rhinoplasty in NYC often want more than a smaller or straighter nose — they want a result that looks natural, fits their face, and does not compromise breathing. Dr. Mourad evaluates the nose as both an aesthetic and a functional structure, assessing the bridge, tip, septum, nasal valves, skin thickness, prior surgery, and airway before recommending a surgical plan.
Rhinoplasty is surgery of the nose performed to refine its external appearance, improve its function, or both. Through carefully planned incisions — typically a small bridging incision on the columella combined with internal incisions, or internal incisions alone — the underlying bone and cartilage are reshaped, and the soft-tissue envelope is allowed to redrape over the new framework.
It is considered when a patient has a dorsal hump, a wide or off-center bridge, a bulbous, droopy, or asymmetric tip, an over- or under-projected nose, a post-traumatic deformity, breathing difficulty from a deviated septum or narrow nasal valves, or an unsatisfactory result from prior surgery. Aesthetic and functional goals are evaluated together, not as separate operations. For a recent nasal fracture, timing changes the plan — see broken nose repair options.
Modern rhinoplasty is a structural operation. Native cartilage is preserved and reinforced rather than aggressively reduced; when additional support is needed, cartilage grafts — septal, auricular, or costal — provide a durable framework. The goal is a natural-looking nose that fits the patient's face and breathes as well as it looks.
Meet Dr. Mourad
A rhinoplasty surgeon in NYC focused on natural structure, breathing, and long-term support.
Dr. Moustafa Mourad is a dual board-certified Facial Plastic and Reconstructive Surgeon and Otolaryngologist–Head and Neck Surgeon whose New York City practice is focused on the face, nose, sinuses, and neck. For patients considering rhinoplasty in NYC, that combined background matters because the nose is both an aesthetic feature and a breathing organ.
His approach is not to create the same nose on every patient, but to study each person’s bridge, tip, septum, nasal valves, skin thickness, facial proportions, ethnicity, prior trauma, and breathing pattern before recommending a plan. When a patient wants a cosmetic change, he evaluates whether that change can be achieved while preserving structural support. When breathing is involved, he plans septoplasty, turbinate reduction, or nasal valve support only when the anatomy indicates it.
His rhinoplasty philosophy is straightforward: the result should look like the patient, not like surgery. Refinement should be visible in facial balance, profile harmony, nasal tip definition, and airway stability — not in an over-reduced, pinched, or generic nose. Consultations are deliberately educational, so patients are shown what can realistically be changed, what should be preserved, and where the anatomy sets limits.
- Dual board-certified in Facial Plastic & Reconstructive Surgery and Otolaryngology–Head & Neck Surgery
- Practice focused on facial plastic, reconstructive, nasal airway, and sinus surgery
- Teaches fellowship-trained facial plastic surgeons through the AAFPRS fellowship
- Published author with peer-reviewed academic work spanning rhinoplasty, sinus, airway, and reconstruction
- Evaluates cosmetic goals and nasal breathing together, not in isolation
BEST of MANHATTAN
2026
Modern Luxury Best of Manhattan 2026
Recognized for Best Rhinoplasty in Manhattan
Modern Luxury named Dr. Moustafa Mourad of MouradNYC "Best Rhinoplasty" in its Best of Manhattan 2026 medical category. For patients comparing rhinoplasty surgeons in NYC, the recognition reinforces the page's central message: rhinoplasty should be planned around facial balance, breathing, cartilage support, and long-term stability.
Third-party recognition is not a guarantee of outcome. Every rhinoplasty plan is individualized.
02 · Why Dr. Mourad
A surgeon other surgeons trust with their hardest cases.
Dr. Moustafa Mourad begins each consultation with a focused history and hands-on nasal exam that emphasizes both form and airway function. The assessment documents septal position, turbinate size, internal and external valve integrity, tip support, and skin quality. Dynamic maneuvers—such as the modified Cottle test to reproduce lateral wall collapse—help link symptoms to anatomy. When indicated, nasal endoscopy (a small flexible camera exam) visualizes intranasal structures and documents the degree of septal deviation or mucosal turbinate enlargement.
Photographic documentation from standardized views supports three-dimensional planning and patient discussion. Imaging such as computed tomography is reserved for complex airway disease, chronic sinusitis, prior trauma, or suspected occult pathology. Dr. Mourad outlines a stepwise surgical plan listing proposed steps—septoplasty, turbinate reduction, grafting sources, and approach type—and explains the rationale for each choice relative to airway safety and long-term support. He emphasizes individualized decisions rather than formulaic solutions.
Dr. Mourad is board-certified by the American Board of Facial Plastic and Reconstructive Surgery and the American Board of Otolaryngology — Head and Neck Surgery. He also serves as an AAFPRS fellowship director in New York City. These credentials reflect dual training in both airway and aesthetic considerations and inform reconstructive reasoning, particularly in revision cases where scar and tissue loss change technical options. Donor-site implications and graft behavior are reviewed in detail so patients understand risks and trade-offs.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
03 · Ideal Candidates
Who benefits most from rhinoplasty.
Good candidates present anatomic findings that match their stated goals and are medically optimized for elective surgery. Clinically relevant indicators include a deviated septum producing obstruction, valve weakness causing airflow limitation, dorsal excess or deficiency, and tip asymmetry that affects appearance or function. Candidates express realistic expectations and typically have adequate donor tissue when grafting is anticipated. For adolescents, documented skeletal maturity and mature decision-making are required, and counseling addresses growth-related variability.
I
Cosmetic Refinement
You would like to refine the appearance of your nose — a dorsal hump, a drooping, bulbous, or asymmetric tip, a bridge that is too wide or off-center, or a profile that feels out of balance with the rest of your face. The goal is a natural, proportionate nose that still looks like yours.
II
Functional Breathing Concerns
Your breathing is limited by the structure of your nose — a deviated septum, narrowed or collapsing nasal valves, or enlarged turbinates. Functional rhinoplasty restores the airway and is frequently combined with septoplasty or valve support in the same operation.
III
Revision or Complex Anatomy
You have had prior nasal surgery, depleted or weak cartilage, thin or scarred skin, or a post-traumatic deformity. These cases need structural rebuilding — often with cartilage grafting — and a more deliberate plan; see our revision rhinoplasty page.
From the Patient Gallery
Rhinoplasty Before and After Cases
A selection of documented rhinoplasty results from the Manhattan practice — a range of ages, anatomy, and goals. Standardized studio photographs before and after surgery; written photographic consent on file. Results vary by patient; these cases are representative, not predictive.



Medically reviewed by Moustafa Mourad, MD, FACS — dual board-certified Facial Plastic & Reconstructive Surgeon and Otolaryngologist (Head & Neck Surgery).
Last reviewed: June 2026
An Honest Note
When rhinoplasty may not be right for you.
Certain medical and psychosocial factors commonly defer or contraindicate elective rhinoplasty. Active nasal or systemic infection, uncontrolled diabetes, and bleeding disorders increase complication risk and generally require treatment before surgery. Active tobacco or nicotine use impairs mucosal healing and elevates wound complication rates; cessation is advised and may be required for safe surgery. Patients with unstable psychiatric illness or unmanaged substance misuse need additional evaluation and support before elective reconstructive or aesthetic procedures.
Anatomic limitations can preclude acceptable outcomes without escalated reconstruction. Extensive prior septal resection with minimal remaining cartilage or large septal perforations complicate standard grafting and may necessitate costal cartilage harvest and staged repair. Patients unwilling to accept longer recovery, donor-site implications, or the probability of staged operations may not be appropriate candidates for definitive improvement. These realities are discussed transparently to avoid unrealistic expectations.
Skin and soft-tissue conditions influence candidacy negatively when active or severe. Very thin skin with prior contour irregularities can increase the risk of visible defects, while fragile or scarred skin can heal poorly. Active inflammatory skin disease on the nose should be treated before elective surgery. Some patients whose goals are temporary contour change are better served with non-surgical options; when appropriate, these alternatives are presented during consultation as part of shared decision-making.
Expectations misalignment often disqualifies surgery until addressed. Patients seeking guaranteed aesthetic outcomes or immediate return to unrestricted activity without realistic recovery planning are counseled that surgery is inappropriate until expectations align with anatomic realities. If you plan to seek insurance coverage for functional correction, our insurance and functional nasal surgery documentation outlines documentation requirements and typical criteria for coverage.
04 · Approaches
Six paths through one procedure.
Rhinoplasty is not a single operation. Each variant addresses a different anatomy, goal, or prior history.
1 of 6 · Primary Rhinoplasty
05 · Technique
Open vs closed rhinoplasty.
Approach selection balances exposure needs with reconstructive goals and individual anatomy. The open approach uses a small external columellar incision to provide direct visualization of tip cartilages and aid precise graft placement. The closed, or endonasal, approach places incisions inside the nostrils and suits more limited reshaping when access is sufficient. Preservation techniques aim to maintain dorsal continuity and avoid large hump resections when anatomy permits. Each choice affects visibility, scarring, and soft-tissue handling and is justified by specific anatomic factors.
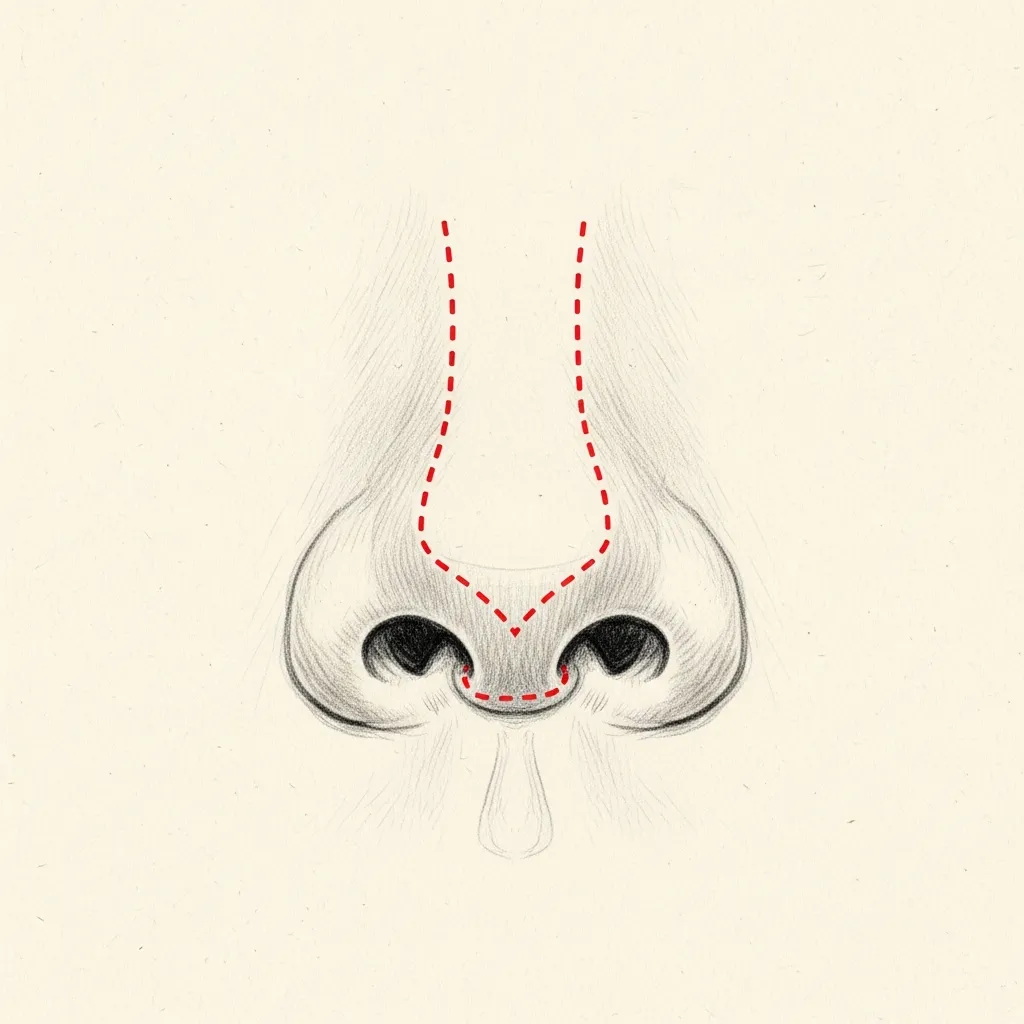
Open
Full Structural Visibility
Structural rhinoplasty focuses on rebuilding long-term support with grafts and anchoring techniques. Common grafts include spreader grafts (thin cartilage pieces placed between septum and upper lateral cartilages to widen the internal valve), columellar struts (supporting pieces between medial crura to stabilize tip projection), and batten grafts (reinforcements for weakened sidewalls). Structural methods are favored when tip stability or valve competence is the primary concern, notably in revision cases where native support is unreliable.
Preservation rhinoplasty preserves native dorsal framework and minimizes soft-tissue disruption, potentially reducing dorsal irregularities in appropriate patients. Preservation is not universally indicated; severe dorsal deviation, prior dorsal surgery, or substantial asymmetry commonly preclude its use. Hybrid strategies often combine preservation-minded dorsal techniques with targeted structural grafting at the tip or valve regions. The decision to pursue preservation depends on preoperative anatomy, airway requirements, and whether preserving continuity will not compromise long-term function.
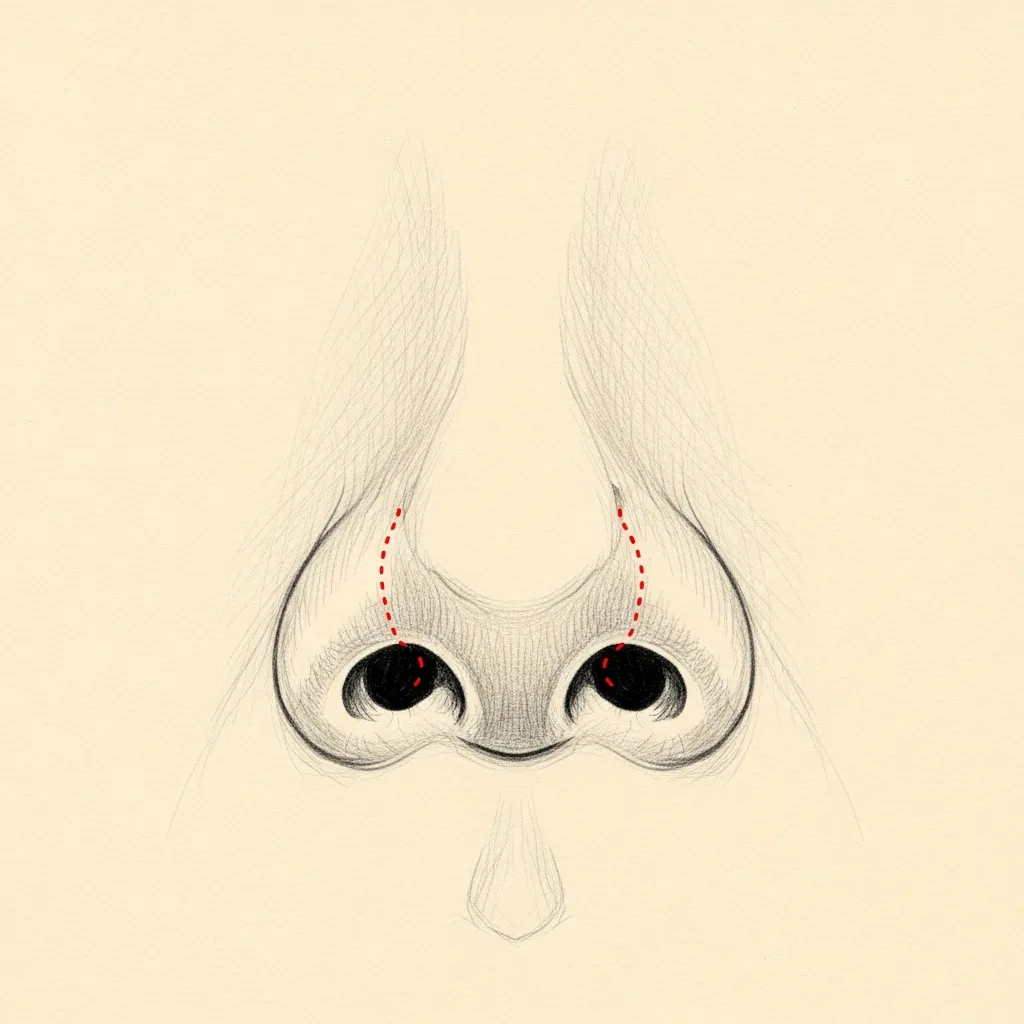
Closed
No External Incision
Graft source selection is case-specific and dictated by availability and mechanical needs. Septal cartilage is preferred when ample stock exists. Auricular cartilage (conchal cartilage) is useful for contouring when septal material is limited. Costal cartilage provides larger volumes and rigidity for major reconstructions or complex revisions. The surgeon discusses donor-site trade-offs, harvest morbidity, and long-term behavior during planning. For further detail on graft selection and dorsal preservation, review preservation rhinoplasty principles.
Illustrative diagrams. Incision design is individualized; the appropriate approach is determined at consultation.
Clinical Rhinoplasty Atlas
Anatomy, balance, and the structures that shape a natural nose
Rhinoplasty is not simply making the nose smaller. It is a structural operation that balances bone, cartilage, skin, facial proportion, and nasal airflow. This atlas explains the anatomy Dr. Mourad evaluates when planning rhinoplasty in NYC, including what can be refined, what must be supported, and what should be preserved.
Select a view, then choose a structure to read what it is and why it matters in planning.
Stylized educational schematic · not a patient image · not to scale
Stylized educational schematic · not a patient image · not to scale
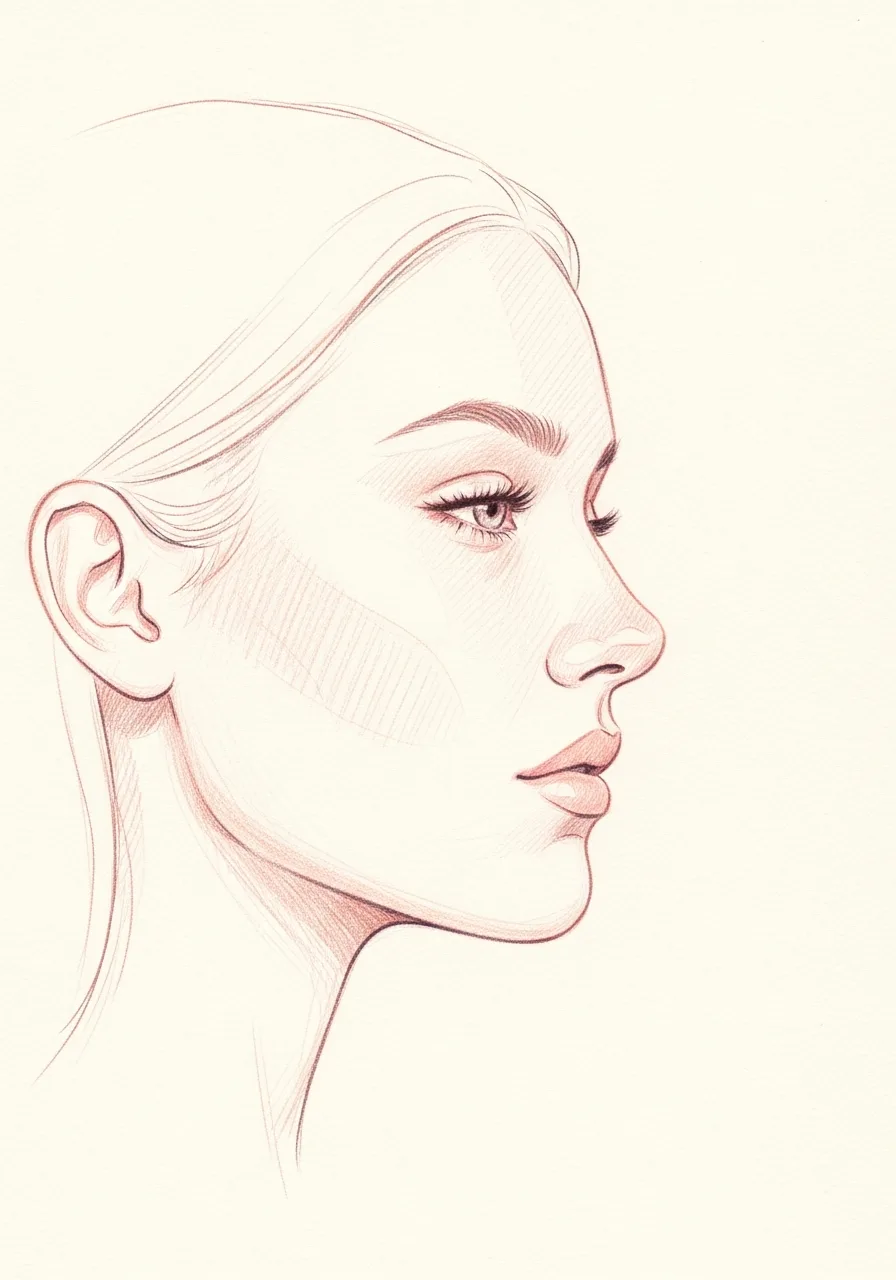
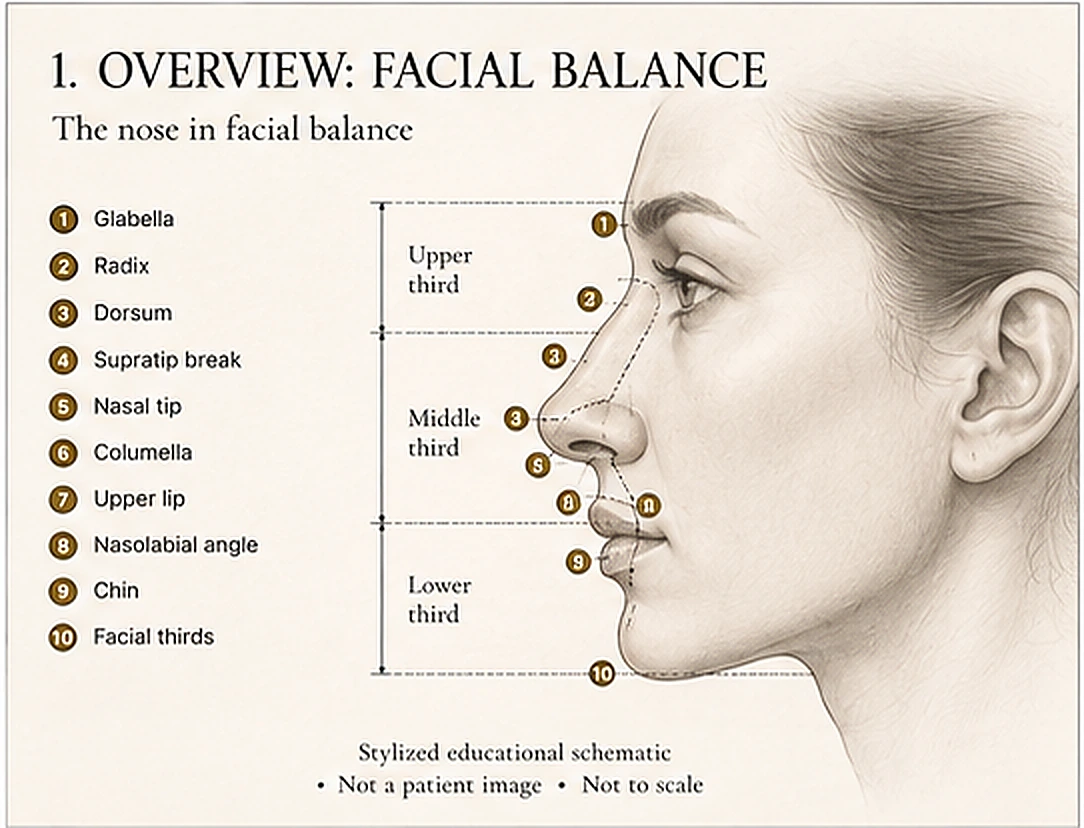
The nose in facial balance
In this view — Shows the nose in relation to the brow, lips, chin, midface, and the vertical facial thirds.
Rhinoplasty planning begins with the whole face, not the nose alone. Dr. Mourad evaluates the nasal bridge, tip, width, projection, rotation, chin, lips, and midface together so refinement looks balanced rather than isolated. The goal is a nose that belongs to the patient's face.
Structure
Glabella
The lower forehead region above the nasal root.
Radix
The transition between the forehead and nose.
Dorsum
The bridge line of the nose.
Supratip break
The subtle transition above the nasal tip.
Nasal tip
The most projecting part of the nose.
Columella
The central tissue between the nostrils.
Upper lip
Affects the perceived nasolabial angle.
Nasolabial angle
The angle between the base of the nose and the upper lip.
Chin
Influences how nasal projection is perceived.
Facial thirds
Vertical balance of the face.
Structures in this view
Stylized educational schematic · not a patient image · not to scale
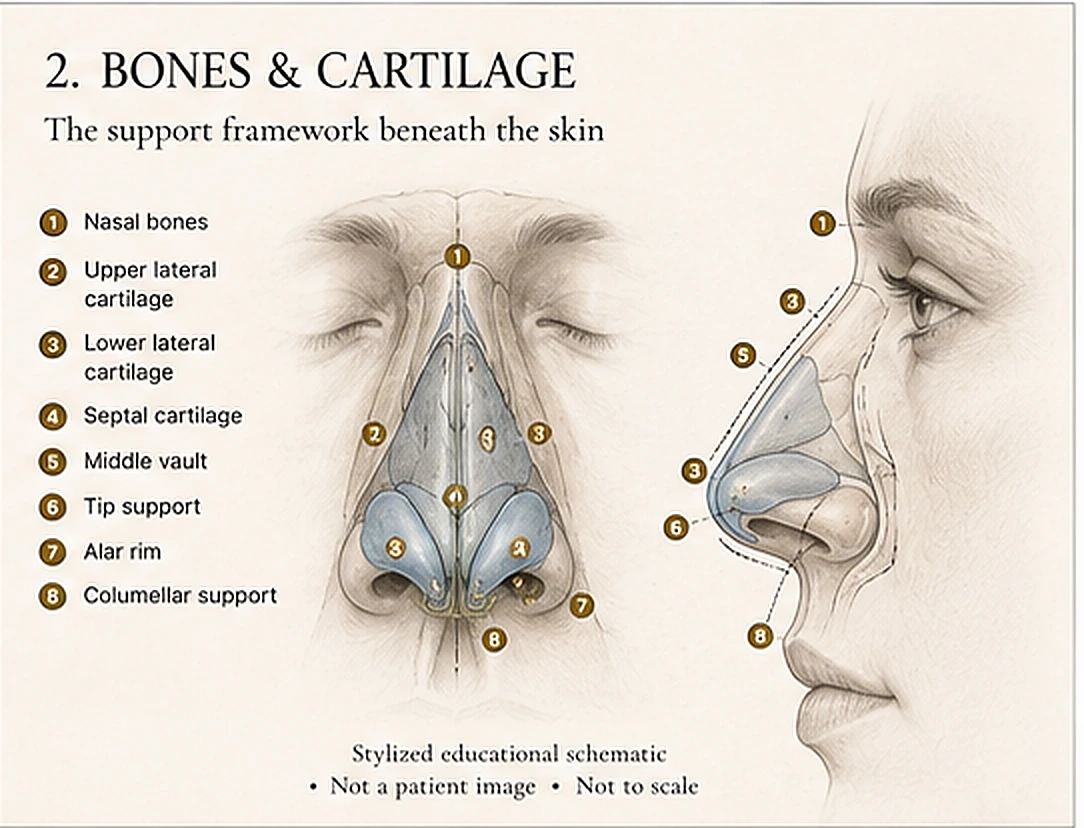
The support framework beneath the skin
In this view — Shows the nasal bones, upper and lower lateral cartilages, septal cartilage, middle vault, and the tip and alar support.
The shape of the nose depends on an underlying framework of bone and cartilage. Rhinoplasty changes must be planned around support. Removing too much cartilage or destabilizing the middle vault can create long-term problems such as pinching, collapse, asymmetry, or breathing difficulty. Dr. Mourad plans refinement with long-term structural stability in mind.
Structure
Nasal bones
Form the upper bridge.
Upper lateral cartilage
Supports the middle vault and internal valve region.
Lower lateral cartilage
Shapes the tip and nostril rim.
Septal cartilage
Central support for both structure and airflow.
Middle vault
Transition zone between bridge and tip.
Tip support
Support system that affects projection and rotation.
Alar rim
Outer nostril rim support.
Columellar support
Central support beneath the tip.
Structures in this view
Stylized educational schematic · not a patient image · not to scale
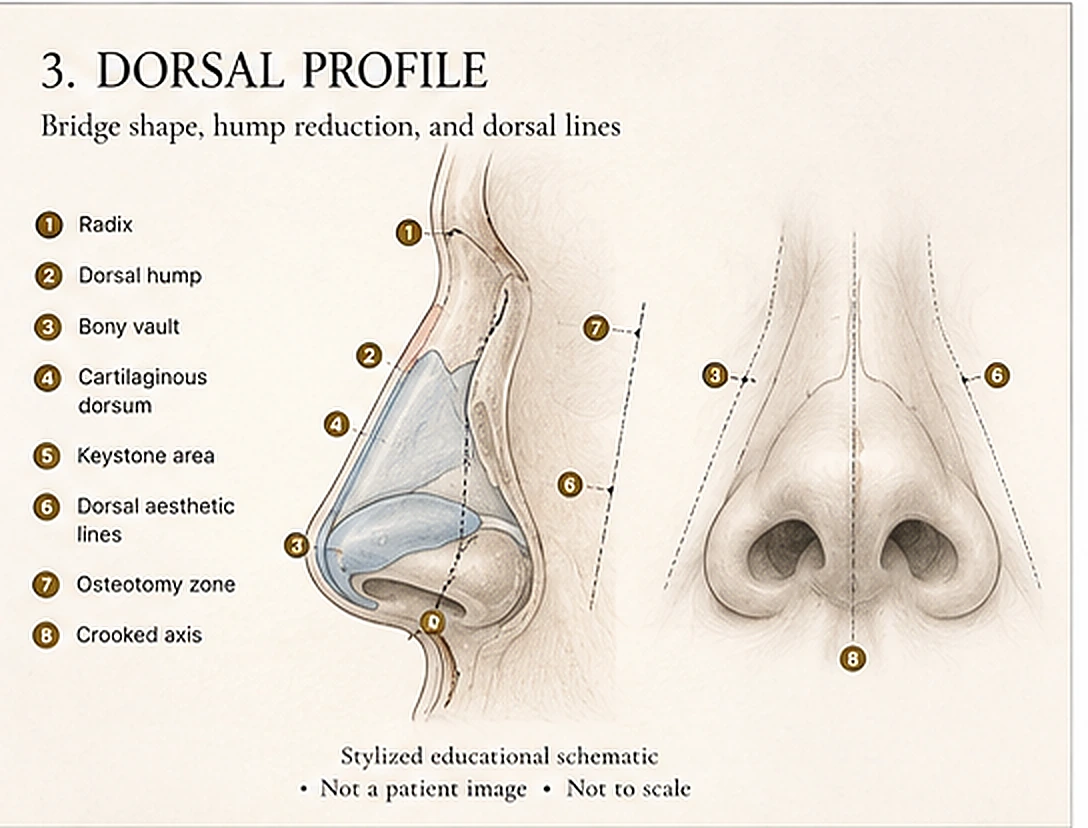
Bridge shape, hump reduction, and dorsal lines
In this view — Shows the radix, dorsal hump, bony vault, cartilaginous dorsum, keystone area, and the dorsal aesthetic lines.
The nasal dorsum defines the bridge line from the radix to the tip. A dorsal hump, wide bridge, crooked bridge, or irregular profile may involve bone, cartilage, or both. Dr. Mourad evaluates whether the safest plan is preservation, structural reshaping, controlled narrowing, or a hybrid approach.
Structure
Radix
Upper starting point of the nasal bridge.
Dorsal hump
Excess height along the bridge.
Bony vault
Upper bridge formed by the nasal bones.
Cartilaginous dorsum
Lower bridge formed by cartilage.
Keystone area
Important transition zone between nasal bones and cartilage.
Dorsal aesthetic lines
Visual lines that define the bridge from the front.
Osteotomy zone
Area where controlled narrowing may be performed.
Crooked axis
Deviation of the bridge from the midline.
Structures in this view
Stylized educational schematic · not a patient image · not to scale
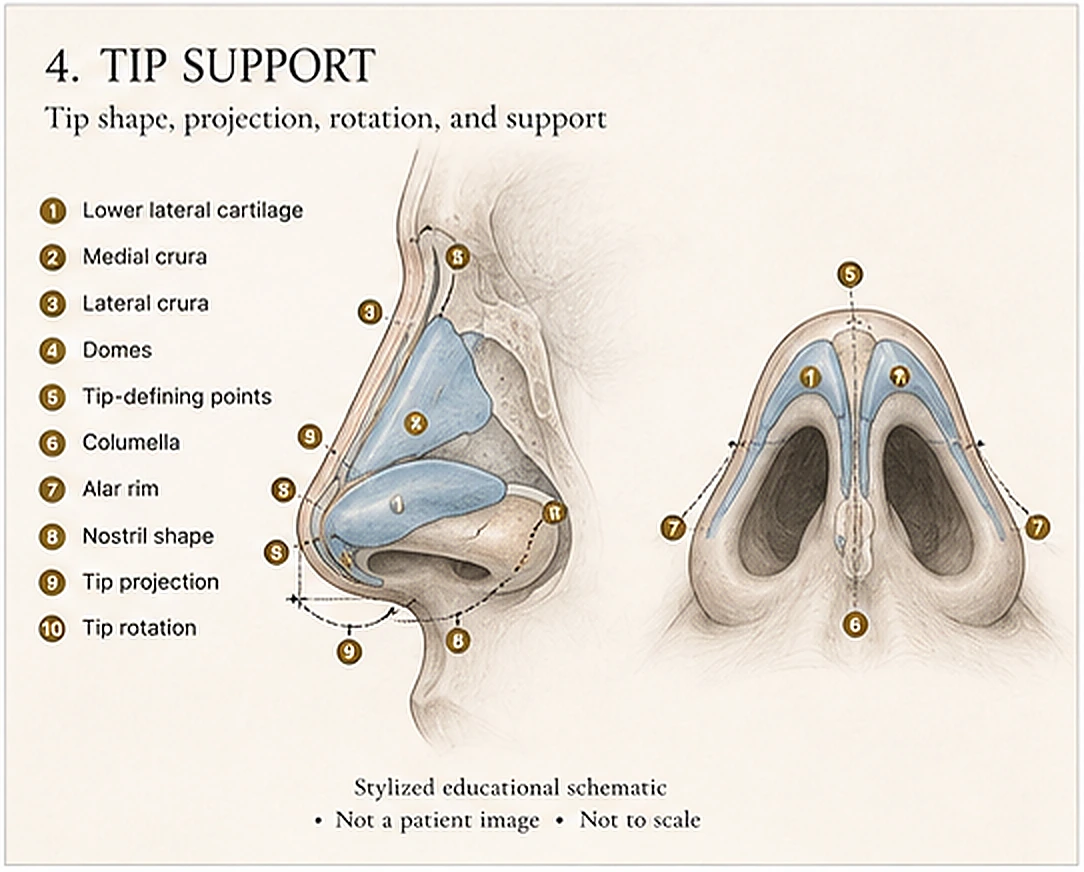
Tip shape, projection, rotation, and support
In this view — Shows the lower lateral cartilages, medial and lateral crura, domes, columella, and the nostril rim.
The nasal tip is shaped by cartilage, skin thickness, projection, rotation, and support. A bulbous, drooping, pinched, under-projected, or over-rotated tip may require very different techniques. Dr. Mourad's goal is refinement without weakening the structures that hold the tip and nostril rim over time.
Structure
Lower lateral cartilage
Main cartilage framework of the nasal tip.
Medial crura
Central support columns of the tip.
Lateral crura
Side portions supporting the nostril rim.
Domes
Tip-defining bend points of the lower lateral cartilages.
Tip-defining points
Visible points that shape tip definition.
Columella
Tissue column between the nostrils.
Alar rim
Outer rim of the nostril.
Nostril shape
Contour influenced by cartilage and skin.
Tip projection
How far the tip projects from the face.
Tip rotation
How upward or downward the tip turns.
Structures in this view
Stylized educational schematic · not a patient image · not to scale
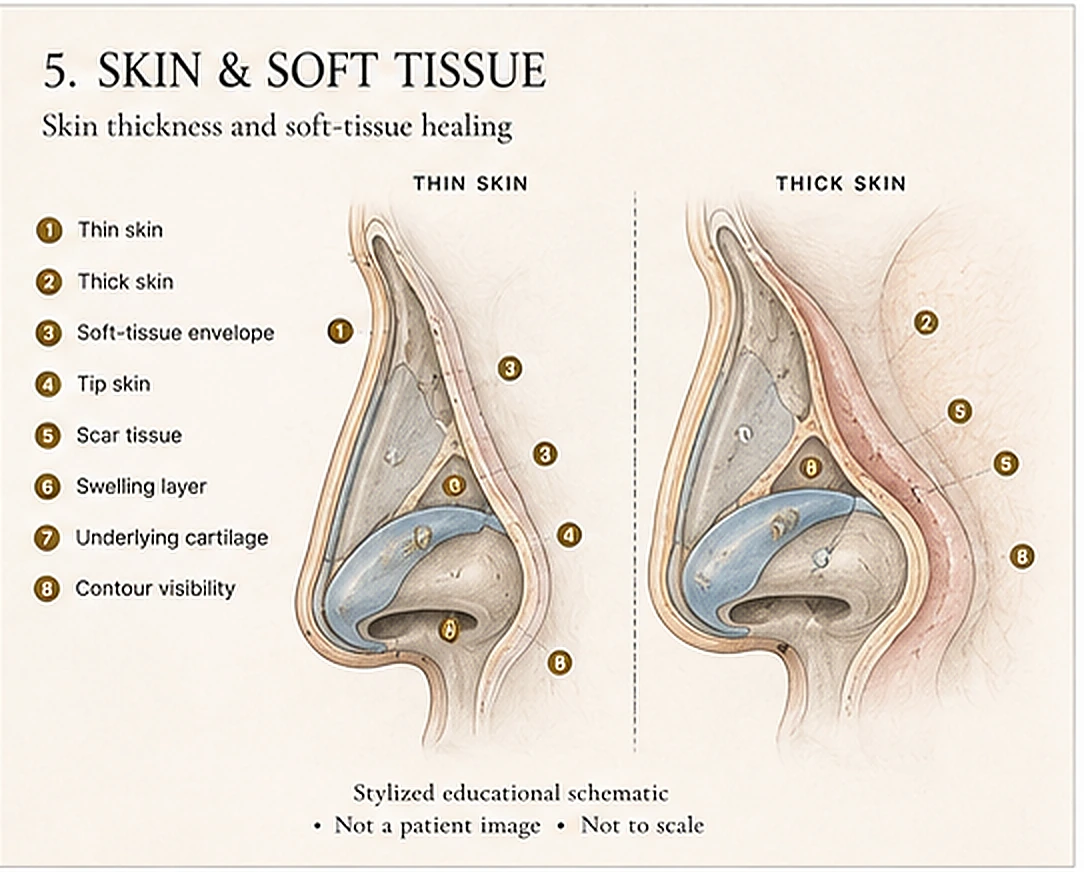
Skin thickness and soft-tissue healing
In this view — Shows the skin and soft-tissue envelope over the cartilage framework, and how thickness affects definition.
Skin thickness affects how much definition is visible after rhinoplasty. Thin skin can reveal small contour irregularities, while thick skin may limit tip definition and hold swelling longer. Revision cases may also involve scar tissue. Dr. Mourad evaluates the skin envelope before setting expectations for definition, swelling, and refinement.
Structure
Thin skin
May show fine contour details and small irregularities.
Thick skin
May limit visible definition and hold swelling longer.
Soft-tissue envelope
Skin and soft tissue covering the nasal framework.
Tip skin
Often the slowest area to refine after surgery.
Scar tissue
More common after prior rhinoplasty.
Swelling layer
Postoperative edema that changes over time.
Underlying cartilage
Framework beneath the skin.
Contour visibility
How much structure is visible through the skin.
Structures in this view
Stylized educational schematic · not a patient image · not to scale
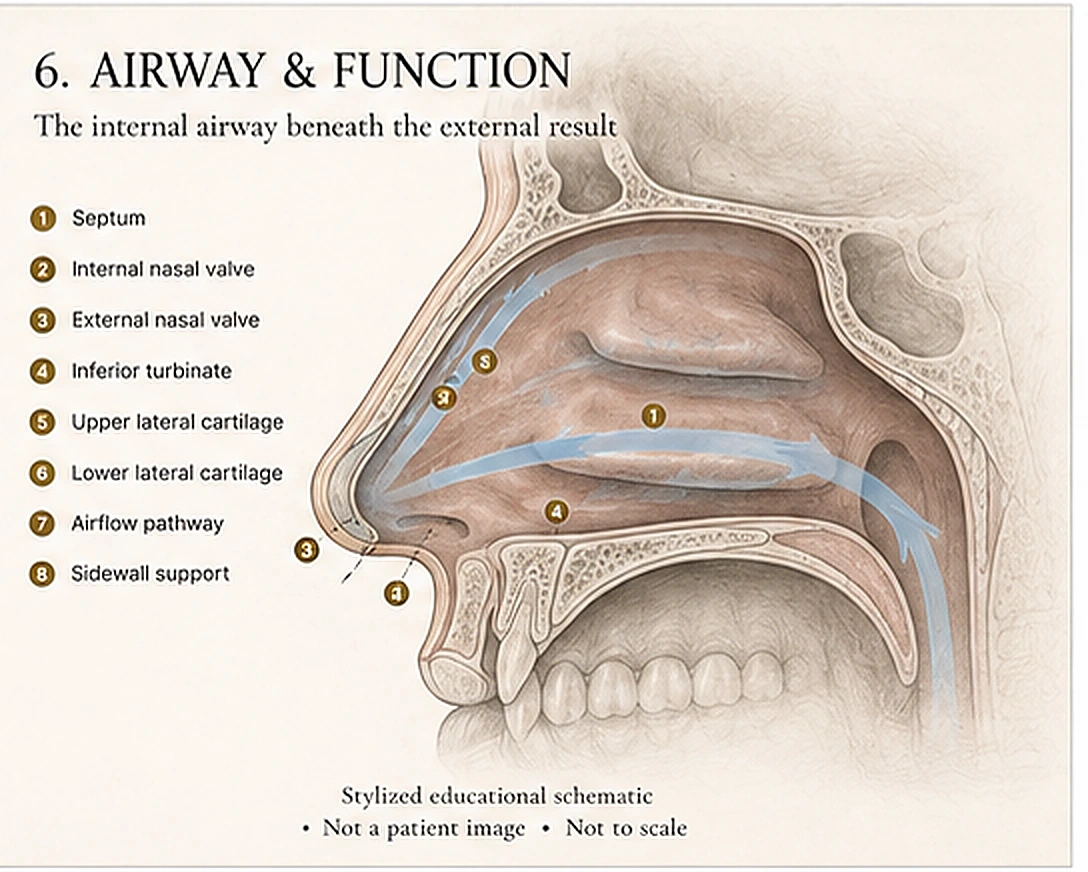
The internal airway beneath the external result
In this view — Shows the septum, internal and external nasal valves, inferior turbinate, and the airflow pathway.
The nose must breathe as well as it looks. Dr. Mourad evaluates the septum, nasal valves, turbinates, sidewall support, and airflow pathway before recommending a rhinoplasty plan. Cosmetic refinement may be combined with septoplasty, turbinate reduction, or nasal valve reconstruction when function is part of the problem.
Structure
Septum
Central wall dividing the nasal passages.
Internal nasal valve
Narrow internal airflow region.
External nasal valve
Nostril-level support zone.
Inferior turbinate
Sidewall tissue that warms and humidifies air.
Upper lateral cartilage
Contributes to internal valve support.
Lower lateral cartilage
Contributes to external valve and tip support.
Airflow pathway
Route air follows through the nose.
Sidewall support
Lateral support that helps prevent collapse.
Structures in this view
What rhinoplasty concerns usually involve
Dorsal hump
Usually involves
Nasal bones, dorsal septum, upper lateral cartilages
Crooked bridge
Usually involves
Nasal bones, septum, dorsal alignment, prior trauma
Bulbous tip
Usually involves
Lower lateral cartilages, skin thickness, tip support
Pinched or collapsed nose
Usually involves
Nasal valves, over-resection, cartilage support
Breathing difficulty
Usually involves
Septum, valves, turbinates, airway passage
How Dr. Mourad uses the atlas during consultation
During consultation, Dr. Mourad evaluates the external shape of the nose and the internal airway together. The anatomy that creates the profile, tip, and bridge also affects long-term support. This is why rhinoplasty planning often includes discussion of cartilage preservation, grafting, septal support, nasal valve stability, skin thickness, and realistic healing.
Structure
The framework that creates the profile, tip, and bridge also determines how the nose is supported over time.
Balance
Refinement is planned against facial proportion, so the nose is considered in relation to the whole face.
Breathing
The septum, nasal valves, and turbinates are evaluated so airflow is protected rather than compromised.
Longevity
Cartilage preservation, grafting, and septal support are planned for durable structural stability over time.
What It Treats
What rhinoplasty can and cannot address.
Rhinoplasty addresses the structure of the nose — bone, cartilage, skin, and airway. It is not a treatment for every concern. Explore common concerns below to see how Dr. Mourad evaluates each one.

Dorsal hump or bridge convexity
Usually yesA dorsal hump or convex bridge can create a prominent profile or distraction from facial balance.
Patients often notice a raised bridge line on profile photographs or feel the bridge dominates the face.
How Dr. Mourad evaluates it
The bridge is assessed from front, oblique, and profile views with attention to the bony vault, cartilaginous dorsum, radix, skin thickness, and facial balance.
Can rhinoplasty help?
Hump reduction, preservation techniques, or structural dorsal refinement may smooth the bridge when anatomy and goals are appropriate.
Limitations
Over-resection can flatten the bridge or destabilize the middle vault; the goal is balanced refinement, not simply making the bridge smaller.
Usually involves
Nasal bones · Cartilaginous dorsum · Upper lateral cartilages · Skin envelope
Related pages
Bulbous or poorly defined tip
Often yesA rounded, wide, or poorly defined nasal tip may reflect cartilage shape, skin thickness, support, or swelling tendency.
Patients often want the tip to look more refined without looking pinched, sharp, or over-operated.
How Dr. Mourad evaluates it
Tip cartilage strength, lower lateral cartilage shape, skin thickness, projection, rotation, and nostril support are evaluated together.
Can rhinoplasty help?
Tip suturing, conservative cartilage reshaping, support grafting, or structural reinforcement may improve definition when appropriate.
Limitations
Thick skin can limit visible definition; aggressive reduction may weaken support and create long-term shape problems.
Usually involves
Lower lateral cartilages · Tip support · Skin thickness · Projection and rotation
Related pages

Wide nasal bridge
Often yesA bridge that appears wide may reflect bony width, dorsal width, facial proportions, asymmetry, or prior trauma.
Patients may notice a broad upper nose from the front or a bridge that makes the nose look heavy or unbalanced.
How Dr. Mourad evaluates it
The bony vault, dorsal aesthetic lines, prior trauma, skin thickness, and relationship to the midface are assessed.
Can rhinoplasty help?
Controlled bony narrowing, osteotomies, or dorsal reshaping may refine the bridge when appropriate.
Limitations
Narrowing must preserve nasal support and airway stability; a very narrow bridge is not always natural or safe.
Usually involves
Nasal bones · Dorsal aesthetic lines · Facial proportions
Related pages

Crooked nose
Often, not always perfectlyA crooked nose may involve the nasal bones, septum, cartilage memory, facial asymmetry, prior trauma, or prior surgery.
Patients often notice deviation in photographs or when the nose does not line up with the rest of the face.
How Dr. Mourad evaluates it
Dr. Mourad evaluates the bony axis, septum, cartilage framework, facial midline, airway, and prior trauma or surgery history.
Can rhinoplasty help?
Septoplasty, spreader grafts, osteotomies, structural support, or septorhinoplasty may improve alignment when appropriate.
Limitations
Complete symmetry is not guaranteed; underlying facial asymmetry and cartilage memory can influence the final result.
Usually involves
Nasal bones · Septum · Dorsal alignment · Cartilage memory · Prior trauma
Related pages

Nasal obstruction
SometimesBreathing may improve when obstruction comes from structural problems such as septal deviation, valve collapse, turbinate enlargement, or post-traumatic deformity.
Patients often want to know whether rhinoplasty can help them breathe better through the nose.
How Dr. Mourad evaluates it
The septum, internal and external nasal valves, turbinate size, mucosa, prior surgery, and sinus symptoms are evaluated together.
Can rhinoplasty help?
Functional rhinoplasty, septoplasty, turbinate reduction, or nasal valve repair may be combined with aesthetic refinement when obstruction is structural.
Limitations
Allergy-related congestion, chronic rhinitis, and sinus disease require separate medical or sinus evaluation and are not corrected by cosmetic rhinoplasty alone.
Usually involves
Septum · Internal nasal valve · External nasal valve · Turbinates · Airway passage
Nasal valve collapse
Yes, when structurally presentNasal valve collapse occurs when the narrowest airflow regions of the nose are weak, narrowed, or collapse during breathing.
Patients may feel blocked despite a straight septum or may notice the sidewall or nostril collapsing inward when they breathe.
How Dr. Mourad evaluates it
Internal and external valves are evaluated dynamically and structurally, sometimes including modified Cottle testing and endoscopy.
Can rhinoplasty help?
Spreader grafts, batten grafts, lateral crural strut grafts, or functional septorhinoplasty may support the airway.
Limitations
Nasal valve repair must be matched to the specific valve problem; septoplasty alone may not correct true valve collapse.
Usually involves
Internal nasal valve · External nasal valve · Upper/lower lateral cartilage · Sidewall support

Deviated septum
Yes, often with septoplastyA deviated septum can narrow one or both nasal passages and may affect both breathing and the visible nasal shape.
Patients may have one-sided blockage, a crooked nose, post-traumatic deviation, or obstruction that does not respond to sprays.
How Dr. Mourad evaluates it
The septum is assessed with history, nasal examination, and endoscopy; imaging is used when clinically relevant.
Can rhinoplasty help?
Septoplasty may be performed with rhinoplasty when the septum contributes to obstruction or supports the external nasal shape.
Limitations
If obstruction also comes from valve collapse, turbinate enlargement, allergies, or sinus disease, septoplasty alone may not solve every symptom.
Usually involves
Septum · Nasal airway · Cartilage support
Related pages

Thick nasal skin
PartiallyThick skin can limit how much fine tip definition is visible after rhinoplasty.
Patients often want a more defined tip but may not realize skin thickness affects how much the cartilage framework shows.
How Dr. Mourad evaluates it
Skin thickness, oiliness, swelling tendency, scar tissue, and underlying cartilage strength are assessed before planning.
Can rhinoplasty help?
The plan often focuses on stronger support, conservative refinement, and realistic expectations rather than aggressive over-resection.
Limitations
Rhinoplasty cannot make thick skin behave like thin skin; definition and swelling timelines vary.
Usually involves
Skin envelope · Soft tissue · Tip support · Swelling tendency
Related pages

Allergies or chronic rhinitis
No, not directlyRhinoplasty does not cure allergy or chronic inflammatory nasal congestion.
Patients may confuse structural obstruction with congestion from allergies, rhinitis, or mucosal inflammation.
How Dr. Mourad evaluates it
Dr. Mourad evaluates lining inflammation, triggers, medication history, turbinate size, and whether symptoms are structural or inflammatory.
Can rhinoplasty help?
Surgery may help if structural obstruction is also present, but medical management remains important for allergy or rhinitis.
Limitations
Medical therapy, sprays, allergy testing, immunotherapy, or rhinitis treatment may still be needed.
Usually involves
Mucosa · Turbinates · Inflammation · Allergy triggers
Related pages

Sinus infections
Only if sinus disease is presentSinus symptoms require separate evaluation; sinus surgery is not performed unless symptoms and imaging support it.
Patients may describe facial pressure, congestion, drainage, or repeated infections and assume rhinoplasty will treat them.
How Dr. Mourad evaluates it
Sinus history, nasal endoscopy, medical therapy response, and CT imaging when appropriate help determine whether sinus disease is present.
Can rhinoplasty help?
Rhinoplasty may be combined with sinus surgery only when both nasal structure and sinus disease require treatment.
Limitations
Rhinoplasty alone does not treat sinusitis, nasal polyps, fungal sinusitis, or recurrent sinus infections.
Usually involves
Sinus drainage pathways · Mucosa · Sinus openings
Related pages

A celebrity nose or a different identity
NoThe goal is facial balance and safe anatomy, not copying another person's nose.
Patients may bring inspiration photos, but the safest result must fit their own face, skin, support, and airway.
How Dr. Mourad evaluates it
Facial proportions, anatomy, skin thickness, airway, goals, and realistic expectations are reviewed together.
Can rhinoplasty help?
A plan can use reference photos to understand preferences, but the result should preserve identity and protect function.
Limitations
Dr. Mourad does not recommend changes that compromise the airway or create an unnatural result.
Usually involves
Facial balance · Identity preservation · Expectations · Safe anatomy
Related pages
06 · In Dr. Mourad's Words
Rhinoplasty videos.
Patient testimonials and short educational films from the Manhattan practice.
Rhinoplasty with Dr. Mourad
An overview of Dr. Mourad's approach to rhinoplasty in his Manhattan practice.
Patient Perspective
A patient discusses her experience before, during, and after surgery.
Inside the Consultation
How Dr. Mourad evaluates anatomy, goals, and surgical candidacy.
Planning & Cost
Planning for Rhinoplasty Cost
Primary Rhinoplasty
Primary rhinoplasty performed by Dr. Mourad commonly begins around $20,000, with many cases around $30,000. Selected limited cases may be lower after evaluation; more complex operations may be higher.
Primary rhinoplasty cost in NYCRevision Rhinoplasty
Revision rhinoplasty performed by Dr. Mourad commonly begins around $25,000, with many cases around $35,000. Pricing varies more widely with the complexity of prior surgery.
Revision rhinoplasty cost in NYCEstimated surgeon's fee. These are planning estimates, not quotes or guarantees. A personalized written estimate is provided after an in-person consultation and examination.
The figures shown represent the estimated surgeon's fee. Facility, anesthesia, laboratory testing, medical clearance, imaging, prescriptions, and other services may be billed separately.
MouradNYC is an out-of-network practice. Eligible medically necessary functional components may be submitted to insurance when the patient's plan includes applicable out-of-network benefits and plan requirements are met. Cosmetic portions remain self-pay. Coverage, authorization, deductibles, coinsurance, allowed amounts, and patient responsibility vary by plan and are not guaranteed. Verification and authorization do not guarantee payment.
Pricing last reviewed: June 2026.
07 · Recovery
What healing actually looks like.
Stage 01
First 24 Hours
Day 0, the operative day, and the first 24 hours combine immediate post-anesthesia effects with expected surgical swelling and bruising. Typical symptoms include nasal congestion, light nasal bleeding or crusting, periorbital bruising, and mild to moderate pain controlled with prescribed medication. Patients should rest at home with limited ambulation and avoid bending at the waist, heavy lifting, and straining that raise intrathoracic pressure. Head elevation while sleeping and intermittent cold compresses over the cheeks reduce periorbital edema and discomfort and should be applied as instructed.
Stage 02
Week 1
Between postoperative day four and day seven most patients leave the highest-pain interval and see steady symptomatic improvement. Analgesic requirements commonly taper from prescription opioids or stronger agents to acetaminophen or milder oral medications as directed by the surgeon. External bruising and periorbital discoloration usually begin to fade but residual swelling remains visible, particularly across the nasal tip and dorsum. Nasal congestion persists because internal mucosal edema and crusting continue while the lining re-epithelializes. Expect variable sleep disruption; head elevation and nightly saline sprays help comfort and nasal hygiene during this interval.
Stage 03
Weeks 2 – 4
During weeks two through four most visible bruising has faded and many patients return to low-demand, nonpublic work when comfortable. Tip swelling commonly persists and can obscure fine contour changes; photographic comparison remains the most reliable way to track progress. Sensation across the dorsum and columella (skin between the nostrils) often remains altered; numbness or tingling typically improves slowly over months. Continue saline irrigation and topical emollients for mucosal moisture and crust control. If you note increasing pain, new drainage, or fever, contact the clinic promptly to evaluate for infection or wound issues.
Stage 04
Months 1 – 3
Between one and three months postoperative most early healing has completed and both breathing and external contour show steady improvement. Tip edema is slowest to resolve because cartilage holds fluid and remodels over months; expect residual fullness through this period. Many patients note meaningful improvement in nasal airflow if septal realignment or turbinate reduction was performed, though some intermittent obstruction can persist. Scar tissue remains immature and may feel firm; directed scar massage and topical therapies can soften tissues once incisions are fully epithelialized. Continue sun protection and avoid elective procedures that might stress healing tissues without clearance.
Stage 05
Months 6 – 12
From six to twelve months postoperative slow tissue remodeling largely determines final contour and nasal support. Cartilage gradually relaxes from operative shaping and grafts further integrate with adjacent tissue. Many patients observe substantial reduction in residual swelling by six months, with ongoing refinement through month twelve. Tip definition typically sharpens as edema resolves and scar softens, while dorsal contour settles and subtle irregularities may emerge. Because remodeling is protracted, surgeons avoid early revision and rely on standardized photographic comparison before considering further surgery.
Six Months to a Year
Long-term healing.
Rhinoplasty results evolve through predictable phases rather than appearing immediately. Early postoperative appearance primarily reflects edema and bruising; as soft tissues thin and cartilage remodels, contour refinement follows. By three to six months many structural changes are visible, and by twelve months most patients reach a near-final appearance. The nasal tip is typically the slowest element to refine because cartilage retains fluid and has intrinsic memory that relaxes gradually. Regular standardized photographs at multiple angles help the surgeon and patient objectively monitor maturation and to determine whether secondary treatment is appropriate.
Functional and aesthetic outcomes are interdependent because structural support influences both contour and airflow. Maneuvers that restore or strengthen tip support and valve integrity often stabilize nasal breathing and reduce the risk of late collapse. Conversely, dorsal smoothing or augmentation changes intranasal dynamics and can affect airway behavior. The durability of outcomes depends on tissue quality, reconstructive strategy, and choice of graft material. Autologous cartilage (patient’s septum, ear, or rib) typically integrates and provides long-term support, whereas synthetic materials have different risk profiles that the surgeon discusses in detail during planning.
Subtle irregularities can continue to improve as scars soften and soft tissues thin over many months. Minimally invasive measures, such as temporary hyaluronic acid fillers, are sometimes used selectively to camouflage minor contour defects during the remodeling phase, but they are temporary and do not replace structural support when anatomy is deficient. When late deformity or functional deficit becomes apparent, the surgeon generally favors waiting until tissues have matured, commonly at or beyond twelve months, before undertaking definitive revision. This timing reduces the risk of correcting transient postoperative findings.
Long-term maintenance considers aging, trauma, and progressive tissue change rather than implying permanence. A durable rhinoplasty emphasizes preservation and reinforcement of support structures rather than maximal tissue removal. Periodic clinical follow-up for one to two years after complex reconstruction is reasonable, with longer surveillance when donor-site harvest or staged reconstructions were performed. The surgeon focuses on conservative cartilage use in any secondary procedure to preserve remaining support and to minimize the risk of future compromise.

Safety & Consent
Risks, safety, and informed consent.
Rhinoplasty carries specific risks that the surgeon reviews during informed consent. Early complications include postoperative bleeding and expanding hematoma, wound infection, adverse anesthesia reactions, and delayed wound healing. Later problems may include septal perforation (a through-and-through hole in the nasal septum), persistent or recurrent nasal obstruction, contour irregularity, graft displacement or partial resorption, and the potential need for revision surgery. Olfactory disturbance (changes in smell) and skin envelope problems are possible. Candid surgical planning, meticulous technique, and appropriate patient selection reduce risk but do not eliminate it, and early detection improves management options.
Bleeding prevention focuses on careful intraoperative hemostasis and clear postoperative instructions to avoid Valsalva, heavy exertion, and nose blowing. If significant postoperative bleeding or an expanding hematoma develops, the surgeon evaluates promptly and may perform controlled nasal packing or return to the operating room when indicated. Infection risk is minimized by sterile technique and selective perioperative antibiotics; if infection occurs, management typically includes targeted antibiotics and drainage when necessary. Septal perforation prevention rests on preserving mucosal flaps, avoiding excessive septal resection, and respecting prior surgical anatomy during dissection.
Contour irregularities and persistent obstruction remain common reasons for later procedure. Contour problems can result from asymmetric cartilage reshaping, inadequate graft support, or scar contracture; management options include observation, nonsurgical camouflage with short-term fillers, or structural revision with autologous grafting. Persistent obstruction may arise from residual septal deviation, turbinate hypertrophy (enlargement of the internal turbinates), or internal and external valve collapse. Preoperative airway mapping and intraoperative stabilization techniques aim to address functional and aesthetic goals together. Revision cases involve greater complexity due to scar tissue and prior grafts, and they often require staged reconstruction.
Red flags requiring immediate contact include expanding facial swelling or a tense hematoma, sudden or progressive visual changes, fever above 101.3°F (38.5°C), uncontrolled pain despite prescribed medication, and any wound breakdown or purulent drainage. For breathing difficulty or chest pain seek emergency care. Donor-site specific risks include chest wall pain and pneumothorax after costal cartilage harvest, and ear deformity or persistent numbness after conchal harvest; these are minimized by appropriate harvest technique and postoperative care. All operative decisions and risk discussions occur during an in-person consultation with Dr. Moustafa Mourad.

Before You Arrive
Your consultation, prepared.
Bring photographs of your nose from earlier in life if you have them.
Note any breathing difficulty — when it began, when it is worst.
List any prior nasal surgery, trauma, or related procedures.
Bring questions. Consultations are designed for a real conversation.
Allow 60 minutes; expect a thorough physical examination.
No decisions are made at the first visit — that is by design.
The Most Important Step
Your expert consultation.
To begin planning, request an in-person consultation so Dr. Moustafa Mourad can perform a hands-on anatomic assessment and discuss individualized options. Dr. Mourad is board-certified by the American Board of Facial Plastic and Reconstructive Surgery and the American Board of Otolaryngology—Head and Neck Surgery; he also serves as an AAFPRS fellowship director in New York City. Bring prior operative reports, clear preoperative photographs, and any prior imaging because these materials materially affect reconstructive choices, graft sourcing, and operative risk. Telemedicine can provide initial screening, but definitive operative planning typically requires in-person exam and, when indicated, endoscopic inspection.
In Their Words
From rhinoplasty patients of the practice.
Selected unedited reflections from patients seen at the Manhattan practice. Names abbreviated; identifying details adjusted with consent.
I had wanted to address my nose since high school but waited until I found a surgeon I trusted not to overdo it. Dr. Mourad understood from the first appointment that I wanted a refined version of my own nose, not someone else's.
My side profile bothered me for years. The hump is gone and the bridge is straight, but my nose still looks like it belongs on my face. People say I look rested, not different.
I was very specific that I did not want a tiny or overly scooped nose. I felt heard from the first appointment and the surgical plan reflected what I had actually asked for.
I came in from out of state for a primary rhinoplasty after consulting with three other surgeons. The conversation here was the most candid by far — what could change, what should not, and what the recovery would actually look like.
My breathing through my right side had been compromised since a childhood injury. Combining the septal work with the cosmetic refinement in one operation was the right call.
What I appreciated most was the restraint. Dr. Mourad talked me out of two changes I had asked for that he felt would not age well. A year in, I am grateful he did.
Individual experiences. Results and recovery vary by patient. Testimonials shared with written consent.
Patient Reviews
Rhinoplasty Patient Experiences
Selected public patient reviews. Individual experiences vary.
“almost 5 years post op and i have still never breathed better before this.”
Real patient experiences
Selected public reviews from patients of the practice.
Your privacy matters
We never share personal health information.
Board-certified expertise
Dual board-certified facial plastic and reconstructive surgeon.
Individual results vary. Reviews reflect individual experiences and are not a guarantee of outcome.
A Focused Option
A focused option for selected low-tip concerns.
Some patients are not seeking comprehensive nasal reshaping. When the concern is primarily a low tip or a tip that drops with smiling, Nasalift™ may provide focused tip elevation in the office under local anesthesia. It does not directly reduce a dorsal hump or replace rhinoplasty when broader structural change is needed.
Explore Nasalift™Continue Exploring
Related rhinoplasty resources.
Does rhinoplasty also improve breathing?
It can. Because the structures that shape the nose are the same ones that carry airflow, a rhinoplasty can be planned to refine appearance and restore breathing in the same operation when both are concerns — this is often called a functional rhinoplasty or septorhinoplasty.
When breathing is the only concern, a functional procedure such as septoplasty or nasal valve repair may be more appropriate; the right plan depends on what is found at examination.
What makes a rhinoplasty look natural?
A natural result comes from preserving or rebuilding structural support rather than simply removing tissue, keeping the new shape in proportion with the rest of the face, and respecting the features that make the nose fit the person. Over-resection is what produces the pinched, scooped, or operated look.
This is why modern techniques emphasize repositioning and reinforcing cartilage — the aim is a nose that looks unoperated and breathes well.
How does Dr. Mourad plan rhinoplasty differently for each patient?
Each plan begins with the individual anatomy — skin thickness, cartilage strength, septal position, airway function, and facial proportions — rather than a standard set of maneuvers. The examination maps what should change, what should be preserved, and what the airway requires, and the operation is sequenced around those findings.
Ethnic identity, prior trauma, and functional needs all shape the plan, which is reviewed with the patient before anything is scheduled.
When is rhinoplasty cosmetic, functional, or both?
Rhinoplasty is cosmetic when it changes only the appearance of the nose, functional when it corrects an anatomic breathing problem such as a deviated septum or valve collapse, and both when one operation addresses appearance and airway together. The distinction matters clinically and for insurance, since only documented functional work may be submitted for review.
Many patients seeking a cosmetic change also have an untreated airway problem — identifying both at consultation avoids a second operation later.
Septoplasty in NYCAt a Glance
Rhinoplasty fact snapshot.
- Treats
- The shape and proportion of the nose — bridge, tip, nostrils, and profile — and, when planned together with airway work, structural breathing problems.
- Does not treat
- Skin thickness itself, sinus disease, or breathing problems on its own unless the airway is specifically addressed in the plan.
- Evaluation
- In-person analysis of facial proportions, skin quality, cartilage support, septum, and nasal valves, with photographs and airway examination.
- Related conditions
- Deviated septum, nasal valve collapse, prior nasal trauma.
- Possible combined procedures
- Septoplasty, nasal valve repair, turbinate reduction, chin augmentation for profile balance.
- Recovery summary
- Splint off around one week; most patients return to desk work in one to two weeks, with swelling refining over a year.
- Insurance / functional distinction
- Cosmetic rhinoplasty is self-pay; a documented functional component may be submitted for insurance review — coverage is never guaranteed. This out-of-network practice provides documentation for reimbursement.
- When to seek evaluation
- When the appearance of the nose has bothered you consistently, after nasal trauma, or when appearance and breathing concerns overlap.
Compare your options
Surgery for a blocked nose, side by side
Different structures cause nasal obstruction, and each has a different operation. Select any two options to compare them directly, or open the full table below. The right choice is determined on examination.
What it addresses
Septoplasty: A deviated septum — the wall between the nostrils.
Turbinate Reduction: Enlarged inferior turbinates reducing airway space.
Changes appearance?
Septoplasty: No — purely functional.
Turbinate Reduction: No — internal only.
Incisions
Septoplasty: Hidden, inside the nostril. No external scar.
Turbinate Reduction: Inside the nose, tissue-preserving.
Typical anesthesia
Septoplasty: General or sedation, individualized.
Turbinate Reduction: Often combined with another nasal procedure.
General downtime
Septoplasty: Most desk work resumes within a few days.
Turbinate Reduction: Minimal; frequently done alongside septoplasty.
Insurance
Septoplasty: May be submitted for insurance review when medically necessary and when the patient's plan includes applicable out-of-network benefits.
Turbinate Reduction: May be submitted for insurance review when medically necessary and when the patient's plan includes applicable out-of-network benefits.
View full comparison table
| Attribute | Septoplasty | Turbinate Reduction | Nasal Valve Repair | Septorhinoplasty |
|---|---|---|---|---|
| What it addresses | A deviated septum — the wall between the nostrils. | Enlarged inferior turbinates reducing airway space. | Collapse or narrowing of the nasal valve (sidewall). | The septum and the external shape, together. |
| Changes appearance? | No — purely functional. | No — internal only. | Usually not; focus is structural support. | Yes — functional and cosmetic in one operation. |
| Incisions | Hidden, inside the nostril. No external scar. | Inside the nose, tissue-preserving. | Approach depends on the technique used. | Endonasal or a small columellar incision. |
| Typical anesthesia | General or sedation, individualized. | Often combined with another nasal procedure. | General or sedation, individualized. | General anesthesia, individualized. |
| General downtime | Most desk work resumes within a few days. | Minimal; frequently done alongside septoplasty. | Varies with the technique; discussed at consultation. | A splint for about a week; bruising settles over weeks. |
| Insurance | May be submitted for insurance review when medically necessary and when the patient's plan includes applicable out-of-network benefits. | May be submitted for insurance review when medically necessary and when the patient's plan includes applicable out-of-network benefits. | May be submitted for insurance review when medically necessary and when the patient's plan includes applicable out-of-network benefits. | The functional portion may be submitted for insurance review when medically necessary and when the plan includes out-of-network benefits; the cosmetic portion is self-pay. |
General information only. Anesthesia, downtime, and insurance vary by patient and plan and are determined individually at consultation.
Find your starting point
Which nasal breathing path fits your situation?
Answer three short questions to see which page explains the evaluation most relevant to you. This is educational orientation, not a diagnosis — a clinical examination is how the cause of nasal obstruction is actually determined.
Select an option for each question to see which page fits your situation.
This guide is general educational information, not medical advice or a diagnosis. Only an in-person examination can determine the cause of nasal obstruction and the appropriate treatment.
See all pathways
A combined revision evaluation likely fits
When both breathing and appearance are concerns after previous surgery, the anatomy is already altered and rebuilding structural support is often part of the plan. A revision evaluation looks at what the prior operation changed before anything is recommended.
A revision rhinoplasty conversation likely fits
Changing the appearance of a nose that has already had surgery is a different undertaking from a first operation, because scar tissue and prior changes shape what is possible. A revision evaluation is the right starting point.
A deviated-septum evaluation likely fits
Persistent, constant blockage that does not resolve with sprays or allergy treatment is often related to a deviated septum. Septoplasty is the functional operation that straightens the septum. If you have had prior nasal surgery, revision considerations also apply.
A nasal valve evaluation likely fits
When the side of the nose draws inward on hard inspiration, the nasal valve — the narrowest part of the airway — may be the contributor rather than the septum alone. This is assessed directly on examination.
A turbinate and sinus evaluation likely fits
Congestion that fluctuates with colds, allergies, or facial pressure often involves swollen turbinates or the sinuses rather than the septum by itself. The evaluation looks at the whole airway before any procedure is considered.
A septorhinoplasty conversation likely fits
When breathing and appearance are both concerns, they can often be addressed together in a single planned operation — straightening the septum while refining the external shape — so there is one recovery rather than two.
A rhinoplasty conversation likely fits
When the concern is the shape of the nose, rhinoplasty is the operation that refines it. A consultation focuses on your goals and whether the underlying anatomy supports them.
A revision evaluation likely fits
After previous nasal surgery, a fresh structural evaluation is the right starting point because the anatomy has already been changed once.
Start with a functional nasal evaluation
Your answers point to more than one possible contributor, which is common. A functional nasal examination is how the cause is identified before any treatment is considered.
Why patients trust this practice
Care led by a double board-certified specialist
Double board certified
American Board of Facial Plastic & Reconstructive Surgery and American Board of Otolaryngology — Head & Neck Surgery.
AAFPRS Fellowship Director
Trains fellows through the American Academy of Facial Plastic and Reconstructive Surgery.
Published author
Contributions to the academic literature of facial plastic surgery.
Face, nose & sinus focus
A practice concentrated above the clavicles, including complex revision evaluations.
Frequently Asked
Rhinoplasty NYC FAQs
Cost depends on whether the surgery is primary, preservation-based, or revision, and on factors such as cartilage grafting, septoplasty, anesthesia, and facility fees. Cosmetic work is self-pay; as an out-of-network practice, the functional portion may be submitted to insurance when it is medically necessary and the patient's plan includes applicable out-of-network benefits, though coverage is not guaranteed. See the Rhinoplasty Cost in NYC guide for detail. A personalized written estimate follows an in-person consultation.
Good candidates are adults in stable health with a specific aesthetic or breathing concern — a dorsal hump, a wide or asymmetric bridge, a drooping or bulbous tip, or obstruction from a deviated septum or narrow nasal valves — and realistic, clearly defined goals. Candidacy is confirmed only after a physical examination of the nasal structure and airway.
Yes. When breathing is limited by structural issues such as a deviated septum, collapsed nasal valves, or enlarged turbinates, functional rhinoplasty — often combined with septoplasty or valve support — can address the airway in the same operation as any cosmetic refinement. The degree of improvement depends on the specific anatomy identified during evaluation.
Rhinoplasty reshapes the external nose. Septoplasty straightens the septum, the internal partition that can obstruct breathing. A septorhinoplasty combines both in a single operation, correcting the airway and refining the external shape together rather than as separate procedures.
Any external splint is usually removed about one week after surgery, and most patients return to non-strenuous work within one to two weeks. Visible swelling continues to settle over the following weeks, with strenuous exercise generally resumed after several weeks. Recovery varies by individual and by the complexity of the procedure.
The nose continues to refine as swelling resolves gradually over many months. Most of the change is apparent within the first few months, while subtle settling — particularly in the tip — can continue through the first year, and longer in revision cases. Individual timelines vary.
Yes. Revision rhinoplasty — correcting an unsatisfactory or compromised result from prior surgery — is a focus of the practice. These cases are structurally complex and often require cartilage grafting to rebuild support beneath a thinned skin envelope, with honest counseling about realistic improvement.
Yes. Ethnic rhinoplasty refines the nose while respecting the patient's heritage rather than imposing a single ideal, and accounts for thicker or more variable skin. Autologous cartilage grafts are generally preferred over synthetic implants for predictable long-term structural support.
Preservation rhinoplasty lowers the dorsum as a single intact unit instead of removing and rebuilding the bridge, which can preserve the natural dorsal lines for suitable primary noses. It is not appropriate for every nose; significant tip work, asymmetry, or prior surgery often still calls for a structural approach.
Clinical references
This page draws on published clinical practice guidelines and public-health references. These sources inform general patient education and do not replace an individual evaluation with Dr. Mourad.
- 01Ishii LE, et al. Clinical Practice Guideline: Improving Nasal Form and Function after Rhinoplasty. Otolaryngology–Head and Neck Surgery. 2017;156(2 suppl):S1–S30. AAO-HNSF guideline
- 02U.S. National Library of Medicine (MedlinePlus). Plastic and Cosmetic Surgery. MedlinePlus
This page is for general educational purposes and is not medical advice. Individual results vary, and the information here does not guarantee a particular outcome or surgical candidacy. Surgical planning is determined only after an in-person evaluation with Dr. Mourad. Patient photographs are shown with written consent.