Double Board Certified · AAFPRS Fellowship Director
Neck Lift in NYC — restore the line of the jaw, naturally.
Neck lift in NYC with Dr. Moustafa Mourad: anatomy‑first platysmaplasty and contouring to refine the cervicomental angle and jawline. In‑person consultation required.
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"A defined neck line is the quietest signal of a youthful face."
A Note from Dr. Mourad
"In Manhattan, I meet many patients who tell me they feel their face still looks young — but their neck doesn't. The neck is often the first area to age and the last to be addressed. A thoughtful neck lift can restore a generation of definition without ever looking surgical."
— Dr. Moustafa Mourad, MD
Key takeaways
- A neck lift treats loose skin, separated platysma bands, sub-platysmal fat, and an obtuse neck angle.
- It typically combines a small incision under the chin with incisions hidden behind the ears.
- It is often combined with a lower facelift, since the jowls and neck are the same problem.
- Submentoplasty addresses the central neck; lateral cervicoplasty tightens skin that has migrated laterally.
- Selected younger patients with isolated submental fullness may suit a more limited submentoplasty.
Overview
What is a neck lift?
A neck lift is a surgical procedure that addresses the structural components of an aged or contour-deficient neck: loose skin, separated platysma muscle bands, sub-platysmal fat, prominent submandibular glands, and an obtuse cervico-mental angle. The operation typically combines a small incision under the chin with incisions hidden behind the ears.
It is considered when the neck shows banding, fullness under the chin, jowling at the jawline, or loss of the sharp angle between the chin and the neck — and when non-surgical treatments such as Kybella, RF skin tightening, or weight loss have not produced the change the patient wants.
A neck lift is often combined with a lower facelift, because the jowls and the neck are anatomically the same problem. In selected younger patients with isolated submental fullness and good skin elasticity, a more limited submentoplasty may be appropriate instead.
Meet Dr. Mourad
A neck lift surgeon focused on jawline definition, anatomy, and natural neck contour.
Dr. Moustafa Mourad evaluates the neck the same way he evaluates the face: as a structural system rather than a surface problem. A neck lift in NYC may involve loose skin, submental fullness, platysma bands, loss of the cervicomental angle, jowl contribution, chin support, or a combination of these factors. Because the neck is closely connected to the jawline and lower face, his consultation begins with anatomy rather than a one-size-fits-all procedure recommendation.
As a dual board-certified Facial Plastic and Reconstructive Surgeon and Otolaryngologist–Head and Neck Surgeon, Dr. Mourad works in an anatomic region he knows from both aesthetic and reconstructive surgery. That experience informs his neck lift planning — including when a limited neck procedure is appropriate, when a facelift-and-neck-lift combination is more honest, and when nonsurgical or conservative treatment is the better choice.
His philosophy is to create definition without an operated look. A neck lift should improve the transition from chin to neck, reduce visible banding when present, and refine the jawline while preserving natural movement and facial character. He discusses incision placement, scar concealment, realistic recovery, and the limits of surgery carefully so patients understand whether their concerns come from skin, muscle, fat, chin projection, or lower-face descent.
- Dual board-certified in facial plastic surgery and otolaryngology–head and neck surgery
- Structural approach to jawline, platysma, and neck contour
- Experience balancing neck lift with facelift and chin support when appropriate
- Practice focused on the face, neck, nasal airway, and reconstructive surgery
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
01 · Why Dr. Mourad
Anatomic precision where most surgeons compromise.
Neck contouring techniques lie along a spectrum from minimally invasive, submental‑focused procedures to open neck lifts with lateral release and skin redraping. A limited or "mini" neck lift typically combines targeted submental liposuction and an anterior platysmal plication performed through a small incision beneath the chin. This closed approach reduces visible scarring and suits patients with good skin recoil and isolated submental fullness. It is insufficient for extensive lateral laxity or wide platysmal separation.
Open neck lift approaches use longer incisions—often with postauricular extensions—to permit release of lateral platysma and redundant skin. Structural options within open techniques include anterior midline platysmal suturing (corset or central plication), lateral imbrication, or selective muscle reorientation. Preservation‑oriented strategies emphasize vascular supply and minimal tissue resection to maintain sensation and function. The choice between conservative repositioning and modest resection depends on anatomy and the goal to preserve natural neck movement.
Liposuction alone reduces localized fat but does not reliably tighten skin or eliminate platysmal bands. Energy‑assisted devices (radiofrequency, laser) may be used adjunctively to encourage skin contraction, but their role is complementary when significant laxity requires mechanical support. Patients considering isolated fat reduction should compare expected gains from liposuction with combined muscle repair or skin excision options, and they can review the neck liposuction resource for technique‑specific details (https://www.nycfacedoc.com/neck-liposuction/).
02 · Ideal Candidates
Who benefits most from a neck lift.
A neck lift addresses laxity of the platysma muscle, excess submental fat, and skin descent below the jaw. The best candidates have noticeable change in the neck specifically — and the structural anatomy to tolerate elegant correction.
I
Submental Fullness
Fullness or fatty deposit beneath the chin (the submental region), often resistant to weight loss and stubborn to non-surgical treatments like Kybella.
II
Platysmal Banding
Visible vertical bands running down the front of the neck — separation and laxity of the platysma muscle that becomes more pronounced with age.
III
Lost Jaw Definition
An obtuse cervicomental angle, jowling that extends below the jawline, and loss of the crisp transition between face and neck — the structural signs of midline descent.
Before & After
A representative case.
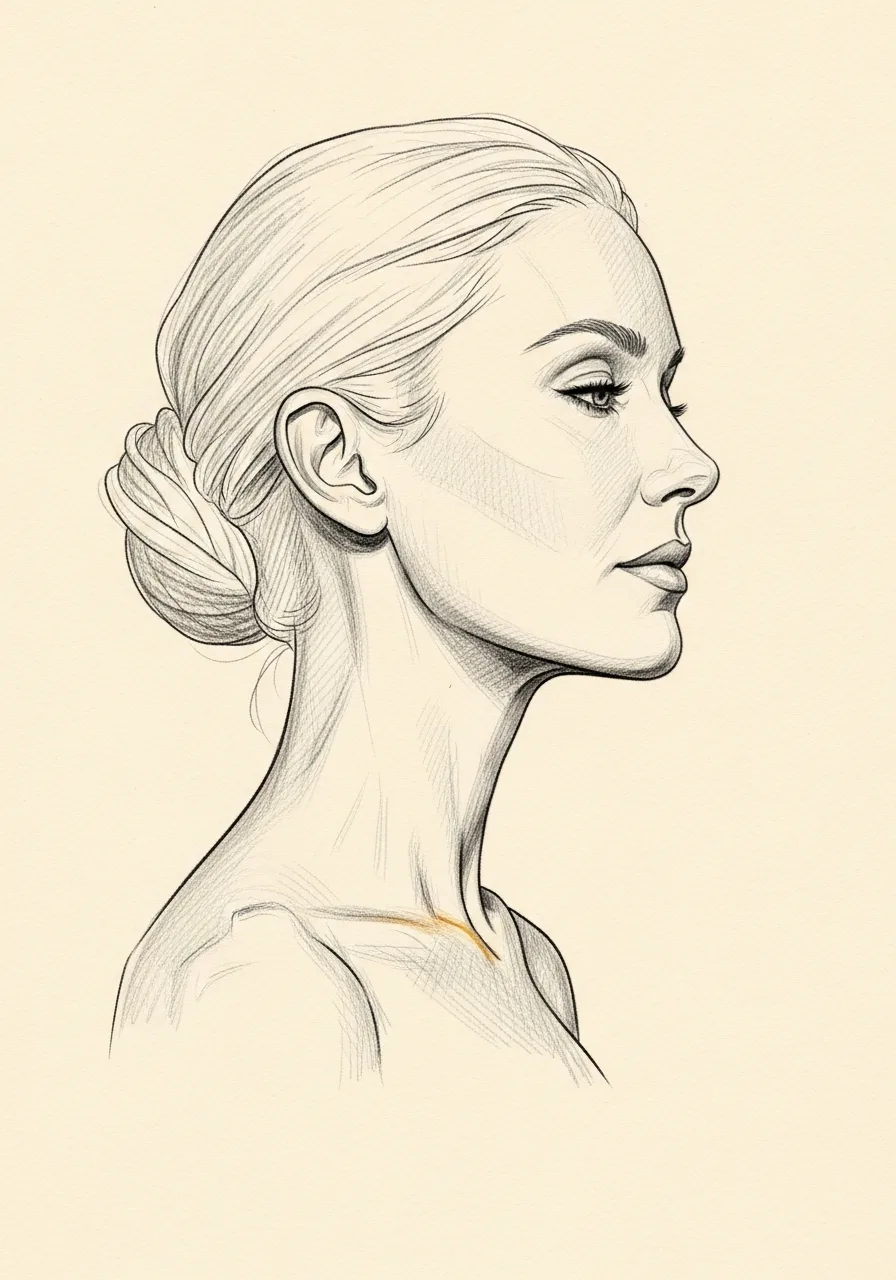
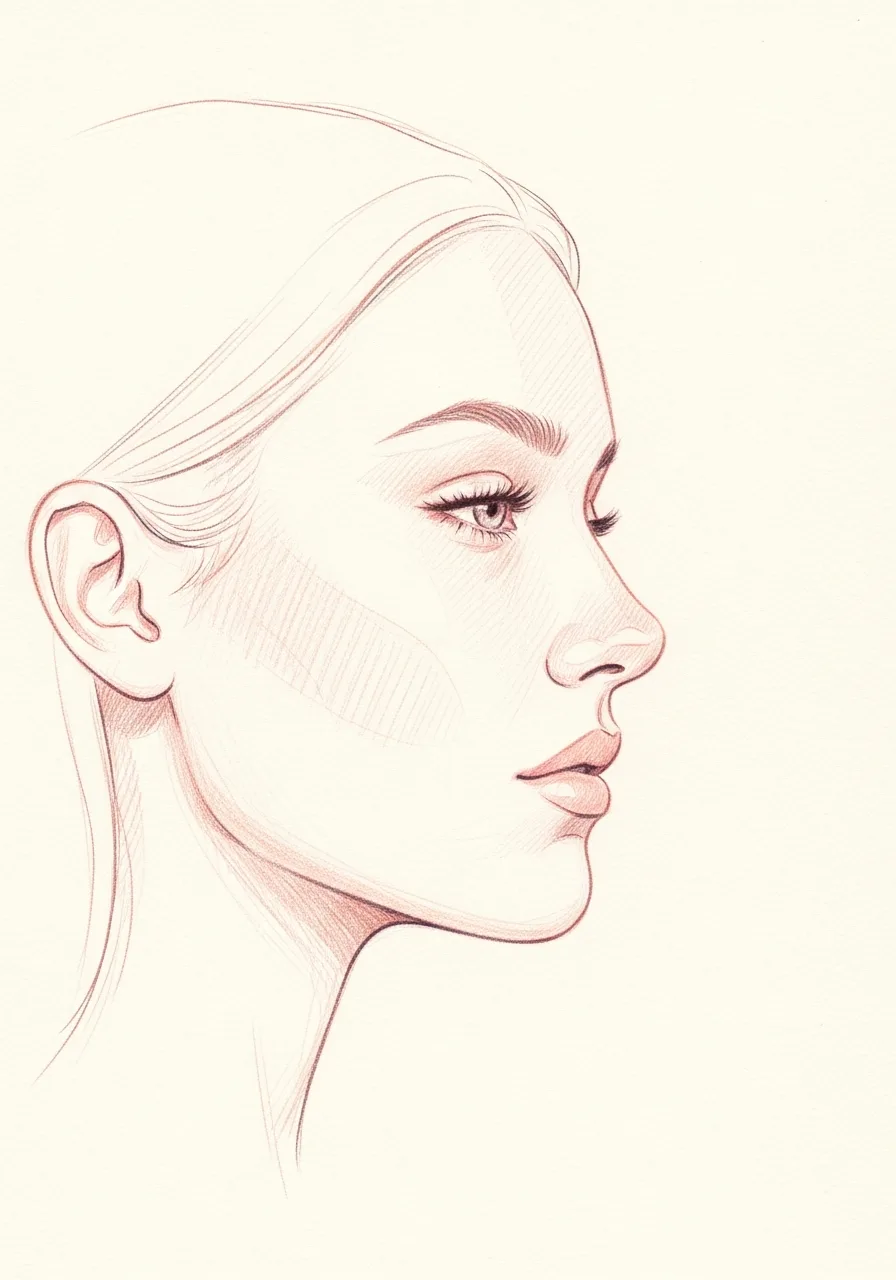
Primary rhinoplasty combined with a neck lift for a female patient in her 30s — note the refined cervicomental angle and jawline definition in profile. Photographed in standardized studio conditions with written consent on file.

Lateral profile · Pre and post-operative comparison · Written consent on file
If this describes you, the next step is a quiet, unhurried conversation — not a sales call.
An Honest Note
When a neck lift may not be right for you.
Patients with isolated mild submental fullness and good skin quality may do better with non-surgical options — Kybella, Coolsculpting, or radiofrequency tightening — before considering surgery.
Significant facial aging that extends well above the jawline is generally addressed together with a facelift in the same operation; a neck lift in isolation can leave the face looking unbalanced.
Active smokers face significantly higher risk of skin necrosis and impaired healing along the neck flap. A nicotine-free window is required.
Patients with unrealistic expectations about how a neck lift can change overall facial appearance benefit from a longer consultation conversation before committing to surgery.
03 · Approaches
Six neck lift techniques.
The right approach depends on which structures are contributing to the change — skin, muscle, fat, or all three. The plan combines the techniques that match the patient's anatomy.
1 of 6 · Submentoplasty
04 · Technique
Submentoplasty vs lateral cervicoplasty.
Neck lift procedures are most commonly performed under general anesthesia in an accredited ambulatory surgery center or hospital, though selected limited procedures can be performed under local anesthesia with intravenous sedation. An anesthesiology professional manages airway and sedation throughout the case. Typical operative time ranges from one to four hours depending on whether adjunctive procedures—chin augmentation or a lower facelift—are performed. The anesthesia plan and perioperative risks are reviewed and documented during the preoperative visit.
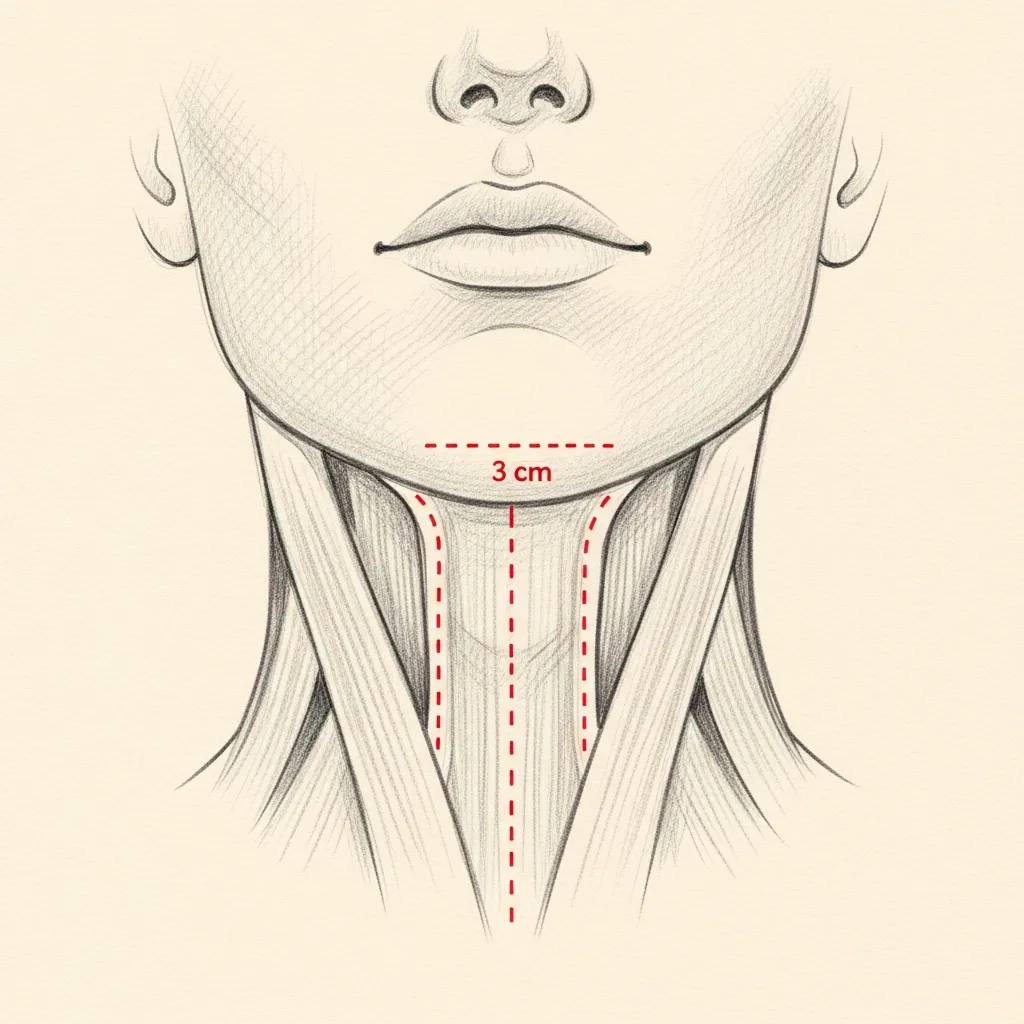
Submental
Through a hidden chin crease
Immediately after surgery patients recover in a monitored area where nursing staff observe vital signs, bleeding, and comfort. Standard immediate measures include a light compressive dressing or chin strap to limit postoperative edema and support the repair. When drains are used, they are typically tunneled discreetly and secured; drain management and expected output are reviewed with the patient and caregiver. Pain control is multimodal and often includes acetaminophen and short courses of prescribed opioids when necessary.
This approach is ideal for patients whose primary concern is midline banding and submental fullness, with good lateral skin elasticity.
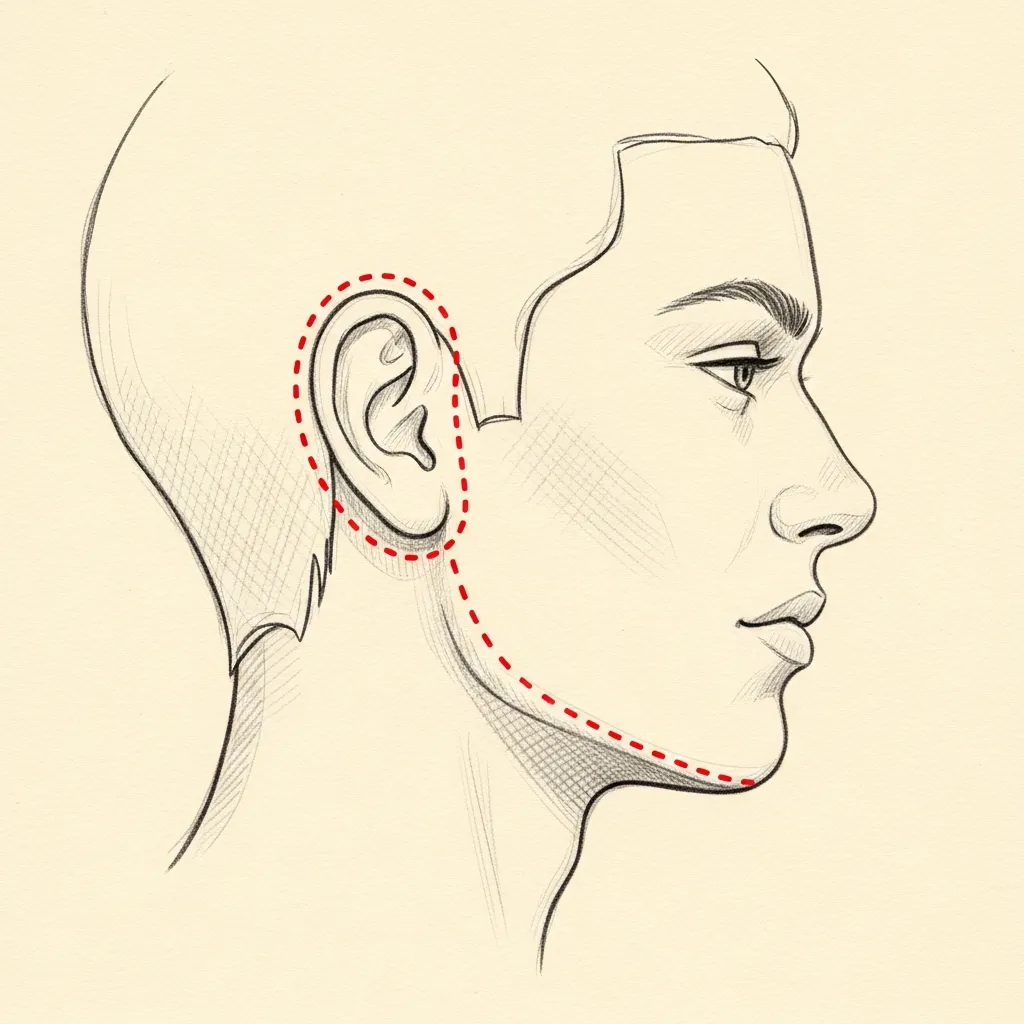
Lateral
Around-the-ear elevation
Meticulous intraoperative hemostasis and postoperative blood pressure control are the primary measures to reduce hematoma risk, a recognized complication of neck surgery. Other immediate risks include wound bleeding, seroma (fluid collection), and transient nerve irritation. To mitigate these, we advise temporary activity restriction, avoidance of medications that increase bleeding risk, and prompt postoperative contact for any expanding swelling, increasing pain, or new weakness. See the clinic patient education page on postoperative hematoma — signs and management (https://www.nycfacedoc.com/postoperative-hematoma/).
The lateral technique is frequently combined with submentoplasty in a single operation to address both midline and lateral changes — and is almost always part of a combined facelift / neck lift in patients with broader lower-face aging.
Illustrative diagrams. Incision design is individualized to the patient's anatomy and combined procedures.
Begin the conversation
A consultation is a clinical evaluation — not a sales conversation.
Cost, Financing & Insurance
Neck Lift Cost, Financing & Insurance in NYC
Neck lift cost depends on the anatomy being treated, including skin laxity, platysmal banding, submental fullness, jawline definition, and whether the neck lift is performed alone or combined with facelift surgery. Some patients need a focused neck procedure, while others benefit from a more comprehensive lower face and neck approach.
A neck lift is generally considered cosmetic and is usually not covered by insurance. After consultation, our office provides a personalized estimate based on the surgical plan, anesthesia, facility setting, and postoperative care. Financing may be available for qualified patients.
What May Affect Cost
- Amount of skin laxity
- Platysmal banding
- Submental fullness
- Whether liposuction is included
- Whether facelift is combined
- Anesthesia and facility fees
This information is educational and is not a guarantee of pricing, insurance coverage, reimbursement, financing approval, or surgical candidacy. A personalized estimate is provided after consultation. Insurance coverage depends on the patient’s plan, medical necessity, documentation, and carrier requirements. Financing terms are determined by third-party financing providers.
06 · Recovery
What healing actually looks like.
Stage 01
First 24 Hours
Day 0, the day of surgery, typically involves postoperative monitoring until patients are stable for discharge, usually within a few hours. Expect tightness across the neck, moderate dull ache, and visible swelling and bruising. A compressive dressing or chin strap may be in place to reduce edema. Oral analgesics are provided for pain control during the first 24 to 48 hours. Ice applied intermittently over the cheeks and submental area can reduce discomfort and swelling, and gentle head elevation while resting is recommended.
Stage 02
Week 1
Day 1 commonly corresponds to peak swelling and bruising for many patients, along with numbness or altered sensation in the submental region and along incision lines. Light ambulation at home is encouraged to reduce venous stasis, but strict restrictions apply: avoid bending at the waist, heavy lifting, straining, and vigorous coughing that can raise blood pressure. Do not drive while taking opioid pain medication. If you have drains, follow instructions for emptying and recording output until the clinic removes them.
Stage 03
Weeks 2 – 4
Days 2 and 3 generally show gradual softening of tightness, though edema and ecchymosis persist. Pain is usually controlled with oral medication that you can taper as comfort allows. If drains remain, they are often removed between postoperative day 1 and day 3 depending on output. Continue to sleep with head elevation and avoid strenuous activities. Keep incisions clean and dry as instructed; showering may be permitted with care, but avoid soaking or hot tubs until wounds are fully healed.
Stage 04
Months 1 – 12
Red flags that require immediate contact or emergency evaluation include rapid unilateral swelling or firmness (possible hematoma), sudden severe pain not relieved by medication, active bleeding through dressings, high fever (over 101.0°F / 38.3°C), shortness of breath, or new weakness of the lower lip or facial asymmetry. For non‑emergent questions about mild redness, transient numbness, or expected drainage, contact the office during business hours. Timely communication helps identify issues such as infection, hematoma, or nerve concerns and permits early intervention when needed.
Have a specific question?
Send a brief note describing your anatomy or concerns — the office will route it directly to Dr. Mourad for review.
Six Months to a Year
Long-term results.
Neck lift results evolve through distinct, measurable phases rather than appearing final immediately after surgery. Early photographs show change but remain confounded by swelling and tissue tightness. Over the first three months the cervicomental angle sharpens as edema resolves and the repaired platysma (the thin superficial neck muscle) integrates with surrounding soft tissue. Scar lines begin to soften between three and six months. By six to twelve months most remodeling is complete and the neck reads as part of the patient’s overall facial proportions, though subtle refinements may continue beyond a year.
Durability relates to underlying structure as much as surgical technique. Adequate chin projection improves perceived neck definition; conversely, a recessed chin can limit visible improvement despite excellent neck surgery. When appropriate, combining a neck lift with chin augmentation (sliding genioplasty or an implant) is considered to balance skeletal and soft‑tissue relationships. Similarly, submental liposuction alone can address isolated fullness but cannot correct significant skin laxity or platysmal banding; review the submental liposuction page (https://www.nycfacedoc.com/submental-liposuction/) for indications and limitations.

Investment
Understanding the value.
Neck lift surgery carries specific, named risks that patients should understand before consenting. Hematoma — a collection of blood under the skin — can present as rapid, tense swelling and requires urgent evaluation because early evacuation reduces skin compromise risk. Seroma (a fluid pocket) may occur and is typically managed with office aspiration or drains. Infection can present with increasing redness, warmth, purulent drainage, or fever and sometimes needs antibiotics or drainage. Contour irregularity, including step‑offs or asymmetry, can require revision surgery once healing and scar maturation are complete.
Nerve injuries are an important category of risk. The marginal mandibular branch of the facial nerve controls lower lip movement and lies near the mandible; injury can cause lower lip weakness, affecting expression and oral competence. Sensory nerves supplying the neck and chin can be stretched or cut, producing prolonged numbness or dysesthesia. Most neuropraxic injuries improve over weeks to months, but persistent deficits are possible and may need electromyography or further management. Meticulous dissection and knowledge of regional anatomy reduce nerve risk but cannot eliminate it entirely.

Before You Arrive
Your consultation, prepared.
Bring photographs of yourself from earlier years if you have them.
Note any prior neck or facial surgery, liposuction, or injectable treatments.
List current medications, supplements, and any blood-thinning agents.
Allow 60 minutes; expect a thorough examination of the neck, jawline, and face.
Bring questions. Consultations are designed for a real conversation.
No decisions are made at the first visit — that is by design.
In Their Words
From patients of the practice.
My neck bothered me in photos more than anything else. After surgery, the change is noticeable but not obvious, which I really appreciate. I feel much more comfortable in pictures now.
I used to angle my face in every photo to hide my neck. Now I don't think about it. The improvement under my chin and along my jawline made a bigger difference than I expected.
I wanted my neck to match how active and healthy I feel. The result is clean and natural, not tight. It gave me back a lot of confidence.
I came from Florida after seeing neck lift results that looked believable. The consultation was very straightforward, and I appreciated that no one overpromised. I'm very happy I made the trip.
Individual experiences. Results and recovery vary by patient. Testimonials shared with written consent.
Patient Reviews
Neck Lift Patient Experiences
Selected public patient reviews. Individual experiences vary.
“My results are natural and stunning.”
Real patient experiences
Selected public reviews from patients of the practice.
Your privacy matters
We never share personal health information.
Board-certified expertise
Dual board-certified facial plastic and reconstructive surgeon.
Individual results vary. Reviews reflect individual experiences and are not a guarantee of outcome.
Frequently Asked
Patient questions, honestly answered.
A neck lift addresses three layers: subcutaneous fat, platysmal muscle, and skin laxity. The procedure can remove or contour submental fat, tighten or reapproximate platysmal edges, and redrape excess skin to restore the cervicomental angle. Chin projection is reviewed because skeletal support affects perceived contour. Individual tissue findings determine which layers are treated; final recommendations are made during consultation with Dr. Mourad.
A neck lift focuses on lower‑neck architecture—platysma, cervicomental angle, and skin immediately under the jaw. Facelift procedures address midface and jowl laxity in addition to the neck and may use different incision patterns. Liposuction removes fat but does not reliably correct platysmal bands or significant loose skin. Your anatomy dictates whether isolated liposuction, a neck lift, a facelift, or a combined plan is appropriate; this is clarified during an in‑office evaluation.
Limited or submental approaches suit patients with primarily fat excess and good skin elasticity and platysmal tone. Full open approaches are indicated when there is lateral platysmal laxity, jowling, or significant skin redundancy. The choice depends on examination findings rather than age alone. Dr. Mourad will explain why a limited or open approach best fits your anatomy during consultation.
Platysmaplasty repairs or tightens the platysma muscle to correct vertical banding and improve midline support. Techniques range from limited plication to formal midline or lateral repairs, chosen based on the pattern of muscle separation. Restoring platysmal support helps maintain a defined jawline and neck contour over time. Specific platysmal strategy is planned after clinical assessment and discussed before surgery.
Most patients have moderate swelling and bruising that peaks in the first 48–72 hours and becomes visibly reduced by 7–14 days. Light activity and short walks are encouraged within 24–72 hours; avoid heavy lifting and vigorous exercise for 4–6 weeks. Subtle settling of tissues and scar maturation continue for 3–6 months. A tailored recovery plan is provided at discharge and reviewed in follow‑up visits.
Incision placement depends on the chosen approach: submental incisions lie in the crease beneath the chin for limited work, while open neck lifts may include discreet periauricular and postauricular extensions to address lateral laxity. Scars are placed to follow natural creases and hairlines when possible and typically mature over 6–12 months. Incision strategy and anticipated scar location are reviewed during preoperative planning so expectations are realistic.
Yes. Chin augmentation—via sliding genioplasty or implant—can improve skeletal projection and optimize the cervicomental angle when chin deficiency is present. Facelift procedures address jowling and midface descent that may otherwise blunt neck results. Combining procedures is often performed in a single operation when safe and appropriate, and the combined plan is determined after in‑person assessment and risk discussion.
Revision neck surgery must contend with scar tissue, altered anatomy, and sometimes deficient skin, which lengthen dissection time and complicate closure. Prior techniques, implants, or excisions influence what can be safely corrected and whether staged surgery is advisable. Revision planning emphasizes realistic goals and careful hemostasis. A thorough review of prior operative records and a focused exam with Dr. Mourad are required before recommending reoperation.
Potential complications include hematoma, infection, prolonged swelling, sensory changes, contour irregularity, poor wound healing, and rare nerve injury affecting motor or sensory function. Hematoma is the complication that most commonly requires urgent attention; management strategies are discussed preoperatively. Specific risk profiles vary with the extent of surgery and patient factors. Risks and mitigation strategies are reviewed during your consultation.
Seek immediate evaluation for expanding neck swelling, sudden breathing difficulty, rapid increase in pain despite medication, active bleeding, high fever, or purulent drainage from an incision. A tense or rapidly enlarging hematoma can threaten the airway and requires urgent attention. For all other concerns, contact the office promptly so Dr. Mourad can advise next steps. Emergency instructions and office contact information are provided at discharge.
Explore Further
Related procedures & resources
Neck rejuvenation is frequently considered together with the lower face and jawline. These pages explain the related options.
Facelift
A neck lift is most often performed as part of a facelift to treat the lower face and neck together.
Read moreBlepharoplasty
Eyelid surgery to complement lower-face rejuvenation.
Read moreChin Augmentation
Improving chin projection can sharpen the jawline and neckline definition.
Read moreBefore & After Gallery
Representative neck lift and facelift cases, photographed with written consent on file.
Read morePatient Reviews
Read experiences from patients of the practice.
Read moreRequest a Consultation
Begin with an unhurried clinical evaluation.
Read moreThe Most Important Step
Your expert consultation.
A neck lift consultation is a careful evaluation of skin, muscle, fat, and bony anatomy. The visit is unhurried, the conversation is honest, and any surgical plan is built around the patient — never the other way around.