Double Board Certified · Reconstructive Nasal Surgery
Septal Perforation Repair — closing one of the most difficult problems in nasal surgery.
Specialized perforated septum repair in Manhattan, including local mucosal flaps, regional flap reconstruction, and free tissue transfer for selected complex defects.
Septal perforation repair in NYC with Dr. Moustafa Mourad for whistling, crusting, bleeding, obstruction, and complex perforated septum reconstruction.
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"Septal perforations are sent to surgeons who have seen them many times. There is very little room for a learning curve."
A Note from Dr. Mourad
"A septal perforation is one of the most technically demanding problems in nasal surgery. Closure depends on tissue size, location, etiology, and the quality of remaining mucosa — every case is individual, and most patients have been told elsewhere that nothing can be done."
— Dr. Moustafa Mourad, MD
Medically reviewed by Moustafa Mourad, MD, FACS — dual board-certified Facial Plastic & Reconstructive Surgeon and Otolaryngologist (Head & Neck Surgery).
Last reviewed: June 2026
Key takeaways
- A septal perforation is a full-thickness opening through both mucosal surfaces and the intervening septal cartilage or bone.
- Symptoms may include whistling, crusting, bleeding, dryness, irritation, and nasal obstruction.
- Not every perforation requires surgery; stable or minimally symptomatic defects may be treated with humidification, saline, ointment, observation, or a septal button.
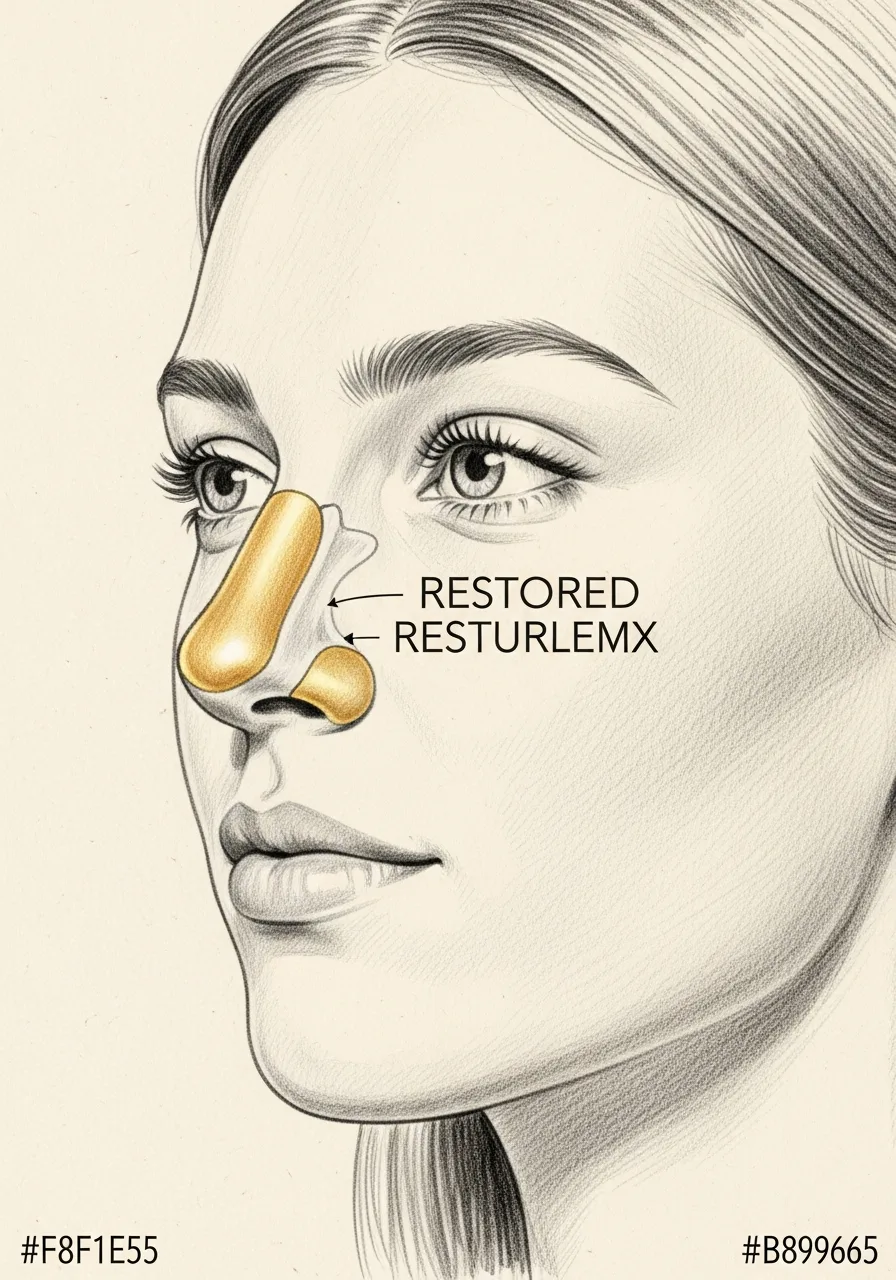
- In Dr. Mourad’s reconstructive algorithm, selected smaller perforations may be repaired with a vascularized local nasal-lining flap based on the anterior ethmoid artery.
- Intermediate or scarred defects may require regional vascularized tissue, including a pericranial flap in selected patients.
- Near-total, total, circumferential, or multiply failed defects may require microvascular free tissue transfer.
- Size is only one factor; location, tissue quality, cause, prior surgery, inflammation, nicotine or intranasal drug exposure, and airway goals may change the plan.
- No technique guarantees closure. The health and blood supply of the nasal lining are as important as the operative method.
Overview
What is septal perforation repair?
Septal perforation repair is reconstructive surgery to close a full-thickness hole through the nasal septum — the internal wall separating the right and left nasal passages. The defect includes the lining on both sides of the septum and may also involve missing cartilage or bone between them.
The goal is not simply to cover the opening. A durable reconstruction must restore healthy lining, reduce turbulent airflow, improve symptoms such as whistling, bleeding, crusting, dryness, and obstruction, and preserve the support and function of the nose.
The reconstructive method depends on how much healthy nasal lining remains. Selected smaller perforations may be repaired with a local vascularized mucosal flap. Larger, scarred, or previously operated defects may require regional vascularized tissue. Near-total or total defects may require microvascular tissue transfer.
Not every septal perforation should be repaired surgically. Small, stable, or minimally symptomatic perforations may be managed with saline, humidification, topical ointment, avoidance of trauma, and observation. A septal button may reduce symptoms for patients who are not surgical candidates or who prefer a non-surgical option.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
01 · Why Dr. Mourad
Diagnosis first, then a plan that fits.
Dr. Mourad has a specific practice focus on septal perforation repair, including cases declined by other surgeons.
Closure technique is matched to the perforation — local flaps, interposition grafts, or in selected cases combined open and endoscopic approaches.
Realistic expectations are set candidly: closure rates depend on size, location, and tissue quality — and a partial improvement is a worthwhile outcome in many cases.
02 · Ideal Candidates
Who benefits most from this operation.
Candidacy is determined together at consultation. The most satisfied patients share three things in common.
I
Symptomatic Perforations
Patients with whistling, crusting, bleeding, or obstruction from a documented septal perforation.
II
Iatrogenic Perforations
Patients whose perforation occurred after prior nasal surgery — often referred from another practice.
III
Non-Active Inflammatory Disease
Patients whose underlying cause (granulomatous disease, vasculitis, or drug-induced injury) is controlled, with stable perforation edges.
From the Patient Gallery
Before & After Septal Perforation Repair
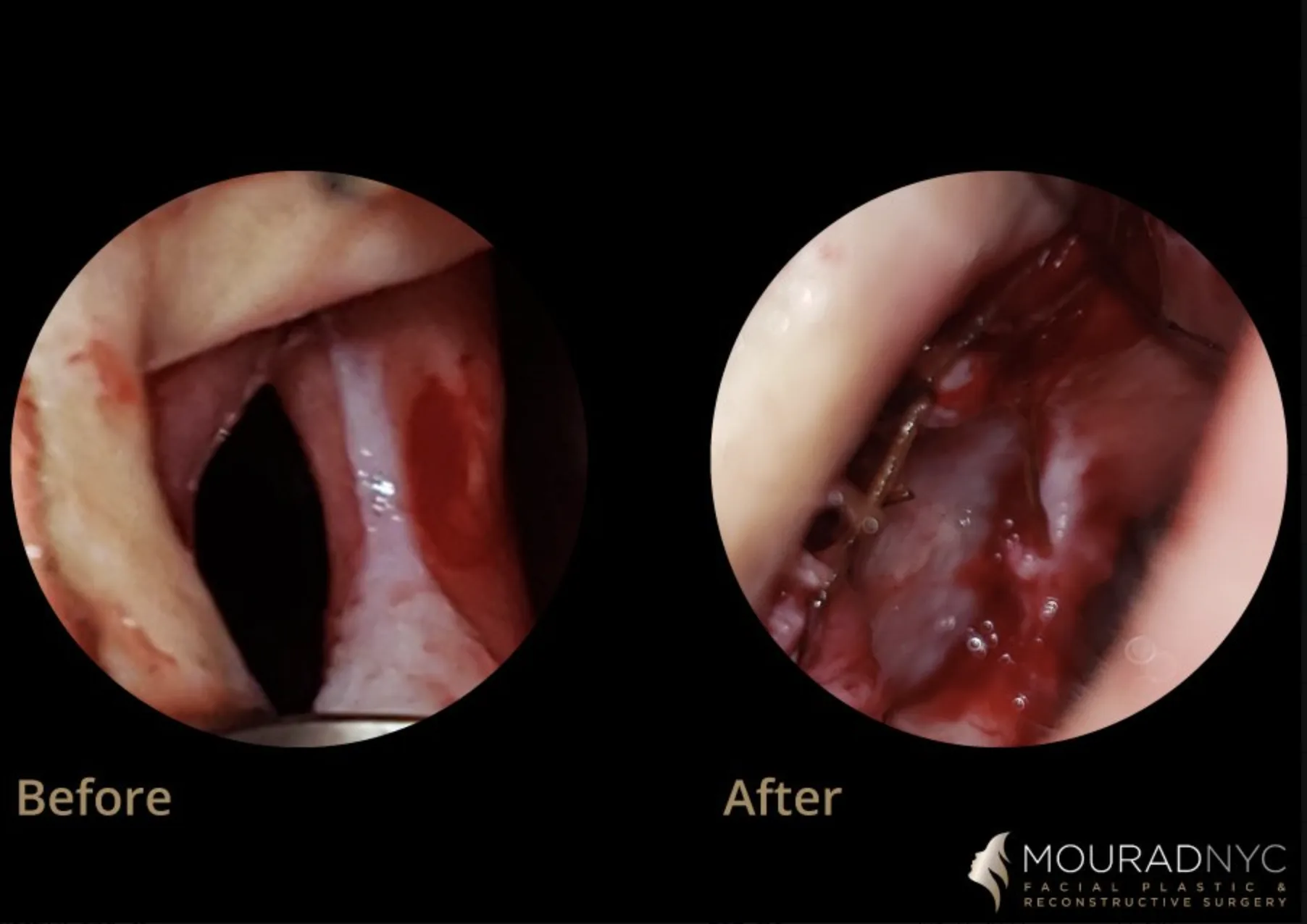
Endoscopic documentation of a septal perforation repair from the Manhattan practice, published with written consent on file. The before view shows the perforation; the after view shows the repaired septum. Individual results vary with perforation size, location, and tissue quality; this case is representative, not predictive.
Septal Perforation Repair ·
Endoscopic before and after documentation of a septal perforation repair. The before view shows the perforation through the septum; the after view shows the repaired septum with the defect closed. Published with written consent on file. Results vary by patient; this case is representative, not predictive.
Pre and post-operative comparison · Photographed in standardized studio conditions · Written consent on file
If this describes you, the next step is a quiet, unhurried conversation — not a sales call.
An Honest Note
When this operation may not be right for you.
Patients with active granulomatous disease, vasculitis, or ongoing intranasal drug use need their underlying disease controlled before repair is attempted.
Asymptomatic perforations may be reasonable to leave alone — repair is not always indicated simply because a perforation exists.
Very large perforations with poor remaining mucosa carry lower closure rates; the conversation about expectations is especially important.
Smokers must stop smoking well before and after surgery — wound healing in the nasal mucosa is uniquely sensitive.
03 · Approaches
Three paths to closure.
Septal perforation repair is one of the most technically demanding operations in nasal surgery. The right approach depends on the size of the perforation, the quality of the surrounding mucosa, and whether closure is the realistic goal.
1 of 3 · Local Mucosal Flap
04 · Treatment Algorithm
How the repair is chosen.
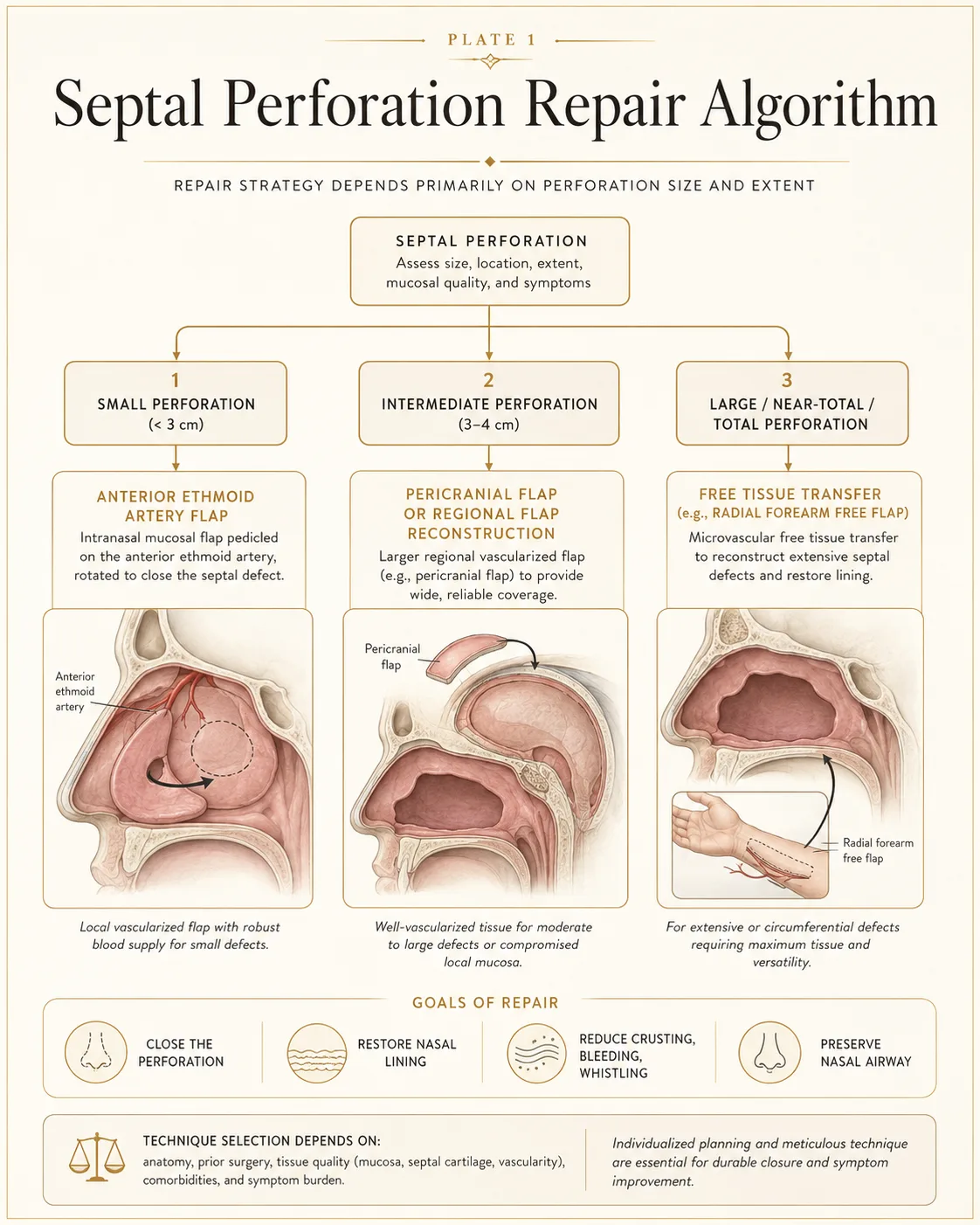
In Dr. Mourad’s reconstructive algorithm, perforation size provides an initial framework, but location, remaining mucosal surface area, vascularity, prior operations, inflammation, underlying cause, and airway goals may alter the final technique. For selected perforations generally under approximately 3 cm, an anterior ethmoid artery-based mucosal flap may be considered when the surrounding nasal lining is sufficiently healthy, mobile, and well vascularized. For perforations roughly in the 3-to-4-cm range, local intranasal tissue may be insufficient, and regional vascularized tissue such as a pericranial flap may be considered. For selected near-total, total, circumferential, or multiply failed defects, microvascular free tissue transfer may be necessary — one option is a radial forearm free flap.
Size is the starting point, not the whole answer. Anterior perforations tend to be more symptomatic than posterior ones; scarred or inflamed mucosa holds a repair less dependably than healthy tissue; and prior operations change what tissue remains available. The goals of every repair are the same: close the perforation, restore the nasal lining, reduce crusting, bleeding, and whistling, and preserve the nasal airway. Which technique can realistically achieve that for a given nose is an individual, anatomical question answered at consultation.
05 · Small Perforations
Local mucosal flap — the anterior ethmoid artery flap.
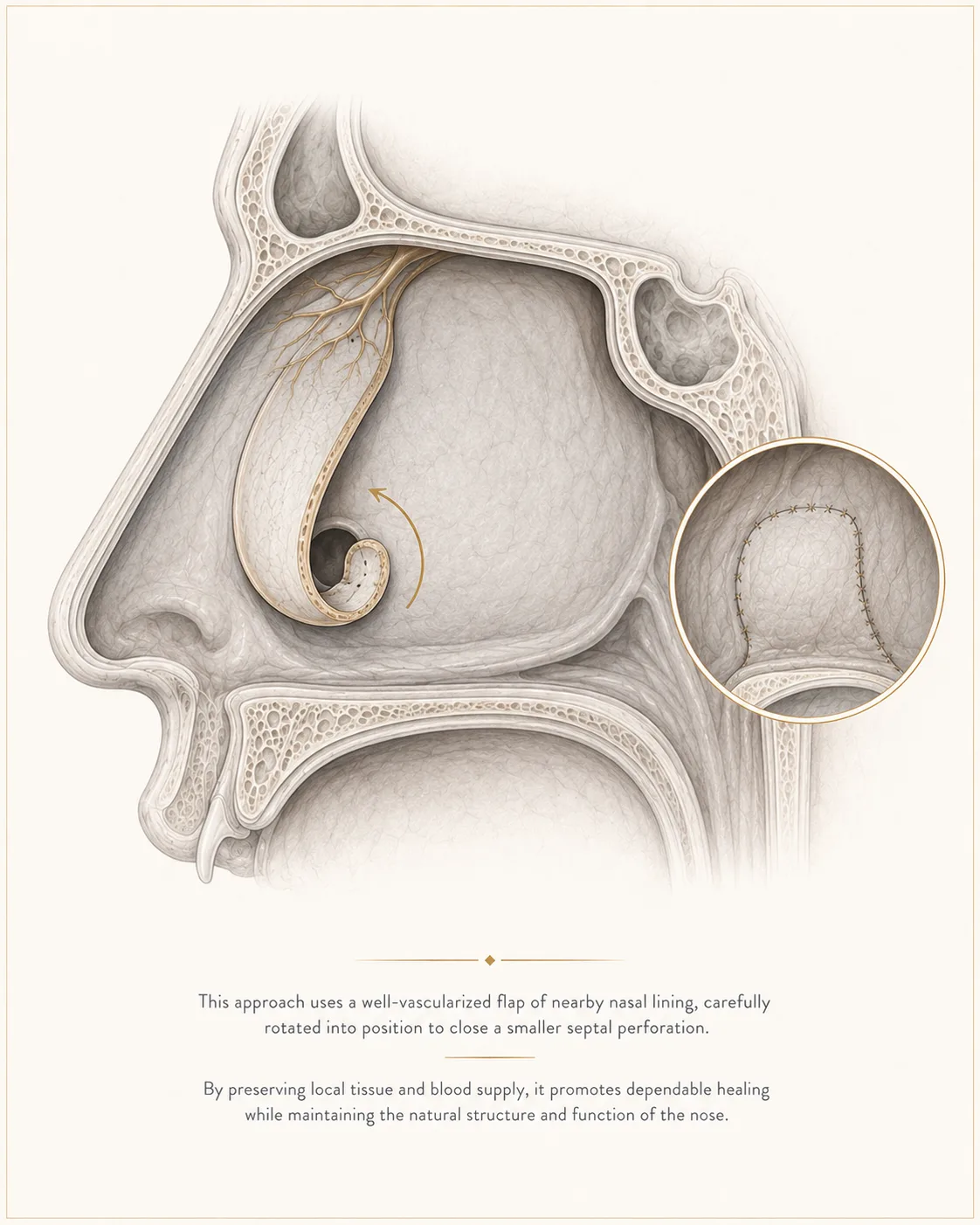
For selected perforations generally under approximately 3 cm, an intranasal mucosal flap pedicled on the anterior ethmoid artery may be considered when the surrounding nasal lining is sufficiently healthy, mobile, and well vascularized. A well-vascularized flap of septal or nasal-wall mucosa is elevated on its arterial pedicle and rotated into the defect, providing healthy local tissue for closure. An interposition graft — commonly temporalis fascia or acellular dermis — may be placed between the mucosal layers as a scaffold while the lining heals. Not every perforation in this size range is a candidate; location, prior surgery, and tissue quality may make another method more appropriate.
Because the flap carries its own robust blood supply, it tolerates the demanding healing environment of the nasal septum better than simple advancement of tissue under tension. Success depends on defect size, tissue quality, prior surgery, vascularity, and control of crusting or inflammation — which is why patient selection and preparation of the nasal lining before surgery matter as much as the operation itself.
06 · Intermediate Perforations
Pericranial and regional flap reconstruction.
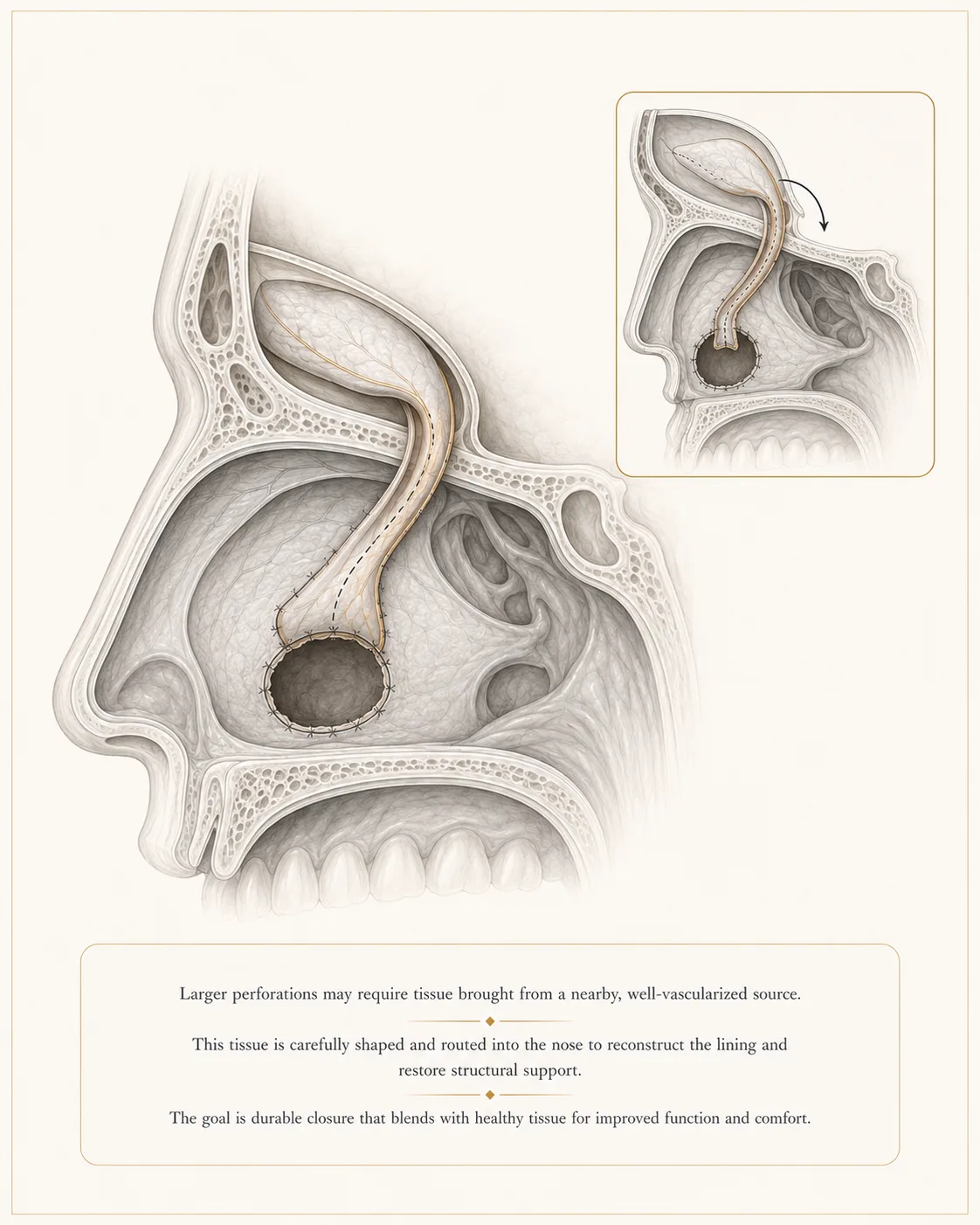
For perforations roughly in the 3-to-4-cm range, local intranasal tissue may be insufficient — the remaining mucosa often will not reach without tension. For these intermediate defects, the reconstructive strategy turns to regional vascularized tissue. One important regional option is the pericranial flap: a thin, well-vascularized layer of tissue from above the skull, tunneled along a transfer pathway near the anterior skull base and brought down to resurface the septal defect from above. Regional reconstruction may also be considered in selected more extensive or revision defects depending on reach, tissue requirements, prior surgery, and available recipient anatomy.
A regional flap brings additional healthy tissue and blood supply into a nose whose own lining has already proven insufficient — which is exactly the situation after failed prior repairs or when the surrounding mucosa is scarred. Other regional options, such as a temporoparietal fascia flap, may be considered when the pericranial flap is not available or not appropriate. Technique choice depends on defect size, prior operations, available mucosa, surrounding support, and whether a regional flap can be transferred safely.
07 · Near-Total & Total Perforations
Free tissue transfer — the radial forearm free flap.
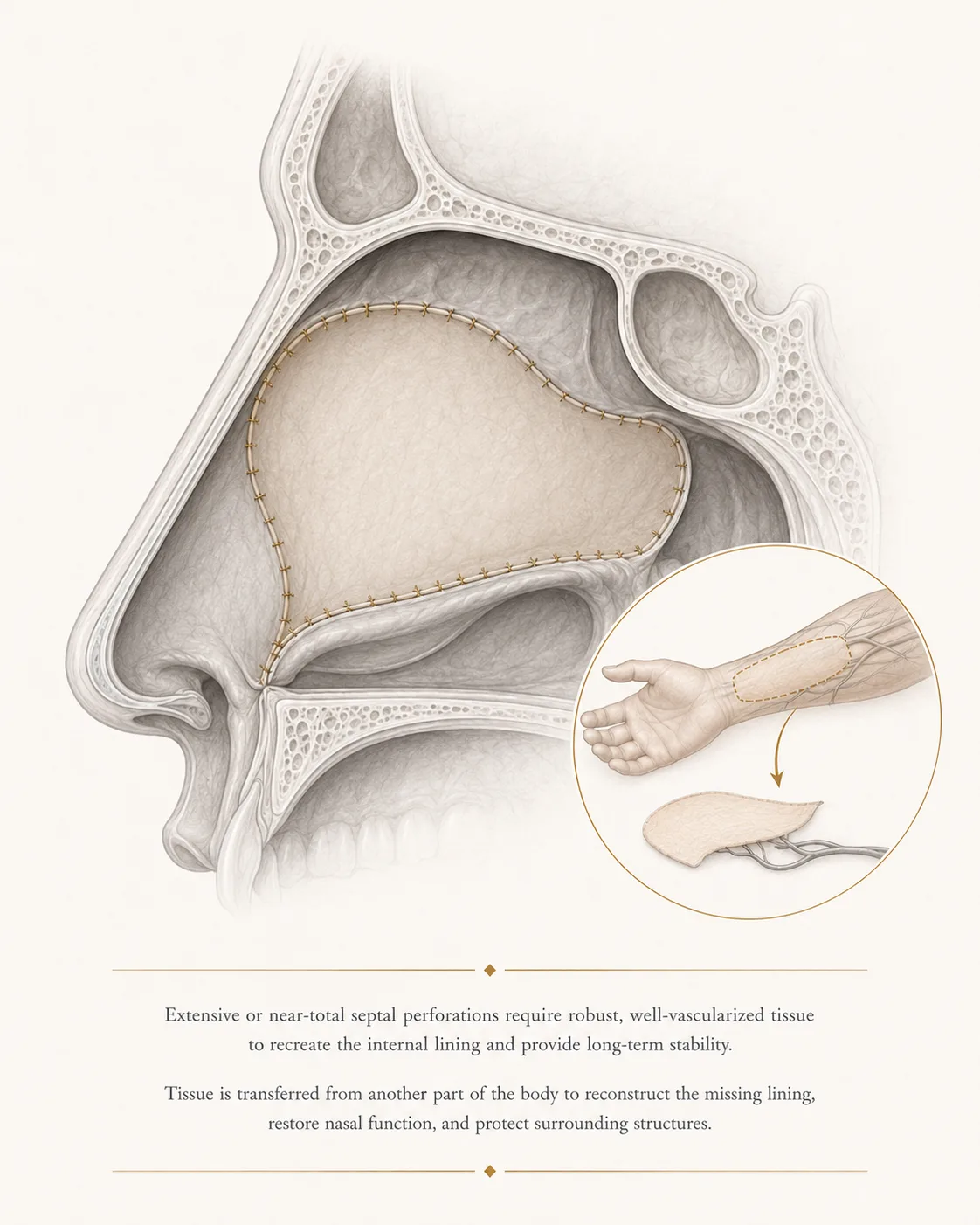
Selected near-total, total, circumferential, or multiply failed septal perforations exceed what local and regional tissue can provide. Reconstruction at this scale may require microvascular free tissue transfer — one option is a radial forearm free flap. A thin, pliable paddle of tissue is harvested from the forearm with its artery and vein, transferred to the nose, and its vessels are reconnected under the microscope to blood vessels in the head and neck.
Free tissue transfer provides a large, well-vascularized lining surface that can reconstruct severe defects and restore the separation of the nasal cavities. These are complex reconstructions that require advanced planning, careful donor-site selection, microvascular technique, and close postoperative monitoring. They are reserved for the most extensive perforations, where the conversation about goals, staging, and realistic outcomes is especially important.
08 · An Honest Note from the Practice
Healing matters as much as technique.
Nasal septal perforations are often associated with impaired blood flow and poor wound healing. These issues may result from underlying autoimmune or inflammatory conditions, chronic nasal irritation, nicotine exposure, intranasal drug use, certain medications, prior surgery, trauma, or other systemic factors.
It is important to understand that the success of a septal perforation repair depends not only on the surgical technique used, but also on the patient's overall health, the quality of the surrounding nasal tissue, and the ability of the nasal lining to heal properly.
Before recommending surgery, we may need to optimize the health of the nasal passages and surrounding mucosa, review previous laboratory testing, obtain a comprehensive autoimmune or inflammatory evaluation, and address any medications, substances, or behaviors that could interfere with healing. Patients may also need to discontinue nicotine, intranasal medications, recreational drugs, or other agents that may compromise blood flow or negatively affect the outcome of the procedure.
The journey toward successful septal perforation repair is often multidisciplinary. It requires a careful, calculated, and deliberate approach that addresses both the perforation itself and the factors that may have contributed to its development. Our goal is not simply to close the perforation, but to create the healthiest possible environment for a durable and successful repair.
Begin the conversation
A careful, honest evaluation is the right first step.
Cost, Financing & Insurance
Septal Perforation Repair Cost, Financing & Insurance in NYC
Septal perforation repair cost depends on perforation size, location, cause, prior surgery, tissue quality, reconstructive technique, grafting or flap requirements, anesthesia, facility setting, and whether additional nasal airway or structural procedures are needed.
MouradNYC is an out-of-network practice. Eligible medically necessary functional or reconstructive components may be submitted to insurance when the patient’s plan includes applicable out-of-network benefits and plan requirements are met. Coverage, authorization, deductibles, coinsurance, allowed amounts, and patient responsibility vary by plan and are not guaranteed. Verification and authorization do not guarantee payment.
A personalized estimate is provided after consultation, once Dr. Mourad has examined the perforation, reviewed prior records when available, and determined which reconstructive pathway is realistic.
What May Affect Cost
- Perforation size and location
- Cause and inflammatory history
- Mucosal quality and scarring
- Primary versus revision repair
- Local versus regional versus free-flap reconstruction
- Graft or donor-site requirements
- Anesthesia and facility setting
- Combined airway or structural procedures
This information is educational and is not a guarantee of pricing, insurance coverage, reimbursement, financing approval, or surgical candidacy. A personalized estimate is provided after consultation. Insurance coverage depends on the patient’s plan, medical necessity, documentation, and carrier requirements. Financing terms are determined by third-party financing providers.
09 · In Dr. Mourad's Words
Educational videos.
Short educational films and patient perspectives from the Manhattan practice.
Dr. Mourad in Practice
An overview of the practice and philosophy.
Patient Perspective
A patient discusses her experience before, during, and after surgery.
Inside the Consultation
How Dr. Mourad evaluates anatomy, goals, and candidacy.
10 · Recovery
Recovery after septal perforation repair.
Stage 01
First Week
Recovery focuses on protecting the reconstructed nasal lining while the flap, graft, or transferred tissue develops a stable blood supply and heals into the surrounding mucosa. In the first week, congestion, mild bleeding, crusting, and pressure are common. Internal splints, silastic sheets, stents, or other supports may be used depending on the reconstruction. Patients must avoid nose blowing, smoke, nicotine, dry air, intranasal trauma, and strenuous activity.
Stage 02
Weeks 2 – 6
The mucosal lining begins to heal across the repair. Saline irrigation, humidification, prescribed ointment, and scheduled endoscopic cleaning may be used to reduce crusting and protect the flap or graft. Follow-up is particularly important during this phase.
Stage 03
Weeks 6 – 12
Mucosalization and tissue maturation continue. Whistling, bleeding, crusting, and obstruction may improve gradually. Healing time depends on the size and location of the original defect, the reconstructive method, tissue quality, and whether additional nasal surgery was performed.
Stage 04
Months 3 – 12
The reconstruction continues to mature. Regional-flap and free-tissue transfer cases may require longer surveillance and, in selected cases, staged refinement. Individual healing varies, and closure or symptom improvement cannot be guaranteed.
Have a specific question?
Send a brief note describing your anatomy or concerns — the office will route it directly to Dr. Mourad for review.

Before You Arrive
Your consultation, prepared.
Bring photographs relevant to your concern, when available.
Bring records from any prior surgery, when available.
List current medications, supplements, and blood-thinning agents.
Note any prior anesthesia issues or chronic medical conditions.
Allow 60 minutes for the first consultation.
Bring questions; no decisions are made at the first visit.
In Their Words
From patients of the practice.
I had crusting and whistling that had become part of my daily life. After the repair, things are much calmer and more comfortable. I'm grateful I finally addressed it.
My septal perforation made me anxious because I didn't know what could actually be done. The explanation was clear and realistic, which helped a lot. I felt taken seriously from the start.
I had seen a few doctors before and still felt confused. This was the first visit where the plan made sense to me. My symptoms have improved, and I'm glad I moved forward.
I traveled to New York because septal perforation repair felt too specialized to choose casually. The process was careful, and expectations were explained honestly. I felt very well cared for.
Individual experiences. Results and recovery vary by patient. Testimonials shared with written consent.
Patient Reviews
Septal Perforation Repair Patient Experiences
Selected public patient reviews. Individual experiences vary.
“I want to start off by saying that dr moustafa mourad has honestly changed my life. I suffered with a perforated septum that was 8mm by 8mm. After being turned down…”
Real patient experiences
Selected public reviews from patients of the practice.
Your privacy matters
We never share personal health information.
Board-certified expertise
Dual board-certified facial plastic and reconstructive surgeon.
Individual results vary. Reviews reflect individual experiences and are not a guarantee of outcome.
Frequently Asked
Patient questions, honestly answered.
No. Septoplasty straightens a deviated septum. Septal perforation repair closes a full-thickness hole through the septum and reconstructs missing nasal lining and, when necessary, structural support.
Size provides an initial framework, but the final plan also depends on location, remaining mucosal surface area, tissue quality, blood supply, cause, prior surgery, inflammation, symptoms, and airway goals.
It is a vascularized flap of nasal lining based on the anterior ethmoid artery. In selected smaller perforations, the flap can be rotated into the defect to provide healthy local lining while preserving its blood supply.
No. The approximate size range is only a starting point. The surrounding mucosa must be sufficiently healthy, mobile, and well vascularized, and location or prior surgery may make another method more appropriate.
A pericranial flap is vascularized tissue from above the skull that can be routed into the nasal cavity. It may provide broader lining coverage when local intranasal mucosa is insufficient.
Microvascular free tissue transfer may be considered for selected near-total, total, circumferential, or multiply failed defects when local and regional tissue cannot provide adequate reconstruction. One option is a radial forearm free flap.
No. Repairability depends on size, location, cause, tissue quality, blood supply, prior surgery, inflammation, and the patient's healing environment. Some perforations are better managed medically or with a septal button.
Repair may reduce whistling, crusting, bleeding, dryness, irritation, and airflow turbulence when those symptoms are caused by the perforation. Individual improvement varies.
Active inflammation, infection, crusting, autoimmune disease, nicotine exposure, intranasal drug use, and irritating medications may need to be addressed before reconstruction.
MouradNYC is an out-of-network practice. Eligible medically necessary functional or reconstructive components may be submitted for insurance review when the patient has applicable out-of-network benefits and plan requirements are met. Coverage and payment are not guaranteed.
Clinical references
This page draws on published clinical practice guidelines and public-health references. These sources inform general patient education and do not replace an individual evaluation with Dr. Mourad.
- 01Cavada MN, Orgain CA, Alvarado R, Sacks R, Harvey RJ. Septal Perforation Repair Utilizing an Anterior Ethmoidal Artery Flap and Collagen Matrix. Am J Rhinol Allergy. 2019;33(3):256–262. Am J Rhinol Allergy
- 02Endoscopic repair of nasal septal perforation with anterior ethmoidal artery flap using tunnel technique. Eur Arch Otorhinolaryngol. 2024. Eur Arch Otorhinolaryngol
- 03Endoscopic Techniques for Nasal Septal Perforation Repair: A Systematic Review. Ann Otol Rhinol Laryngol. 2023. Ann Otol Rhinol Laryngol
- 04Surgical repair of nasal septal perforations: A systematic review and meta-analysis. Int Forum Allergy Rhinol. 2022. Int Forum Allergy Rhinol
- 05Total septal perforation repair with a pericranial flap: radio-anatomical and clinical findings. Laryngoscope. 2018. Laryngoscope
- 06Mobley SR, Boyd JB, Astor FC. Repair of a large septal perforation with a radial forearm free flap. Ear Nose Throat J. 2001;80(8):512. Ear Nose Throat J
- 07Surgical repair of large nasal septal perforation: a systematic review and meta-analysis. Eur Arch Otorhinolaryngol. 2026. Eur Arch Otorhinolaryngol
- 08Microsurgical Repair of Large Nasal Septal Defects. Ann Plast Surg. 2025. Ann Plast Surg
Explore Further
Related conditions & procedures
Septal perforation repair sits within functional nasal surgery. These pages explain the condition and the related operations.
Septal Perforation (condition)
Symptoms, causes, and how size and location guide treatment.
Read moreSeptoplasty
Correction of a deviated septum, sometimes relevant to perforation cases.
Read moreRevision Rhinoplasty
When prior nasal surgery is part of the history.
Read moreSeptorhinoplasty
Combined functional and structural nasal surgery.
Read moreRequest a Consultation
Begin with an unhurried clinical evaluation.
Read moreThe Most Important Step
Your expert consultation.
A careful evaluation by a double board-certified physician is the right first step. The conversation is unhurried, the diagnosis is honest, and the operative plan is built around what your anatomy can sustain and what you actually want.