Double Board Certified · Revision Rhinoplasty
Pollybeak Deformity — a recognisable post-rhinoplasty problem.
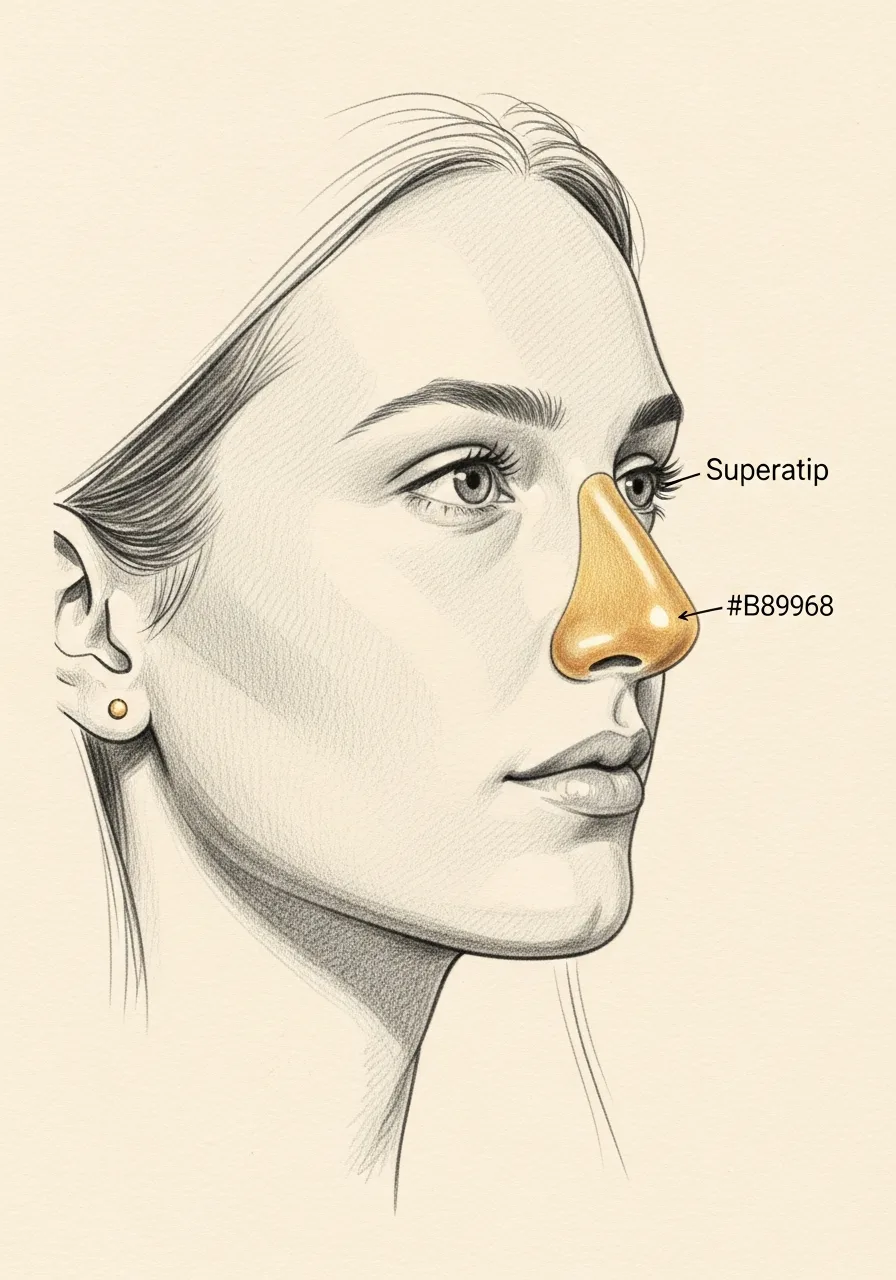
Pollybeak deformity is a convex fullness in the supratip area — the region just above the tip of the nose — that creates a parrot-beak-like profile. It is…
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"A pollybeak is one of the most recognisable post-rhinoplasty problems — and one of the most correctable when evaluated thoughtfully."
A Note from Dr. Mourad
"Pollybeak deformity is a convex fullness in the supratip area — the region just above the tip of the nose — that creates a parrot-beak-like profile. It is most often a post-rhinoplasty problem, with both soft-tissue and structural causes."
— Dr. Moustafa Mourad, MD
Overview
What is pollybeak deformity?
Pollybeak deformity is a post-rhinoplasty contour problem in which the supratip area — the region of the bridge just above the tip — sits too high relative to the tip, producing a convex profile reminiscent of a parrot's beak. The tip can also appear under-rotated and droopy as a secondary effect.
The deformity can be structural, when too much dorsum was left or too much tip support was removed, or soft-tissue, when scar tissue forms in the supratip dead space during healing. Distinguishing the two is essential because their treatments are completely different.
Soft-tissue pollybeak may respond to steroid injections, taping, and time during the first year after rhinoplasty. Structural pollybeak requires revision rhinoplasty to rebalance the dorsum and tip. A careful examination, imaging, and review of operative records guide the choice.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
Castle Connolly Top Doctor — Plastic Surgery, 202602 · Symptoms
How this condition typically presents.
Three patterns are most common. Patients often recognise themselves in one or more of these.
I
Supratip Fullness
Visible convexity in the supratip area, most obvious on lateral profile view, creating a parrot-beak appearance.
II
Lack of Tip Definition
The tip appears under-projected relative to the supratip, blunting the natural tip-defining transition.
III
Persistent After Healing
Fullness that persists beyond the expected post-rhinoplasty swelling period — typically beyond 6 to 12 months.
03 · Anatomy
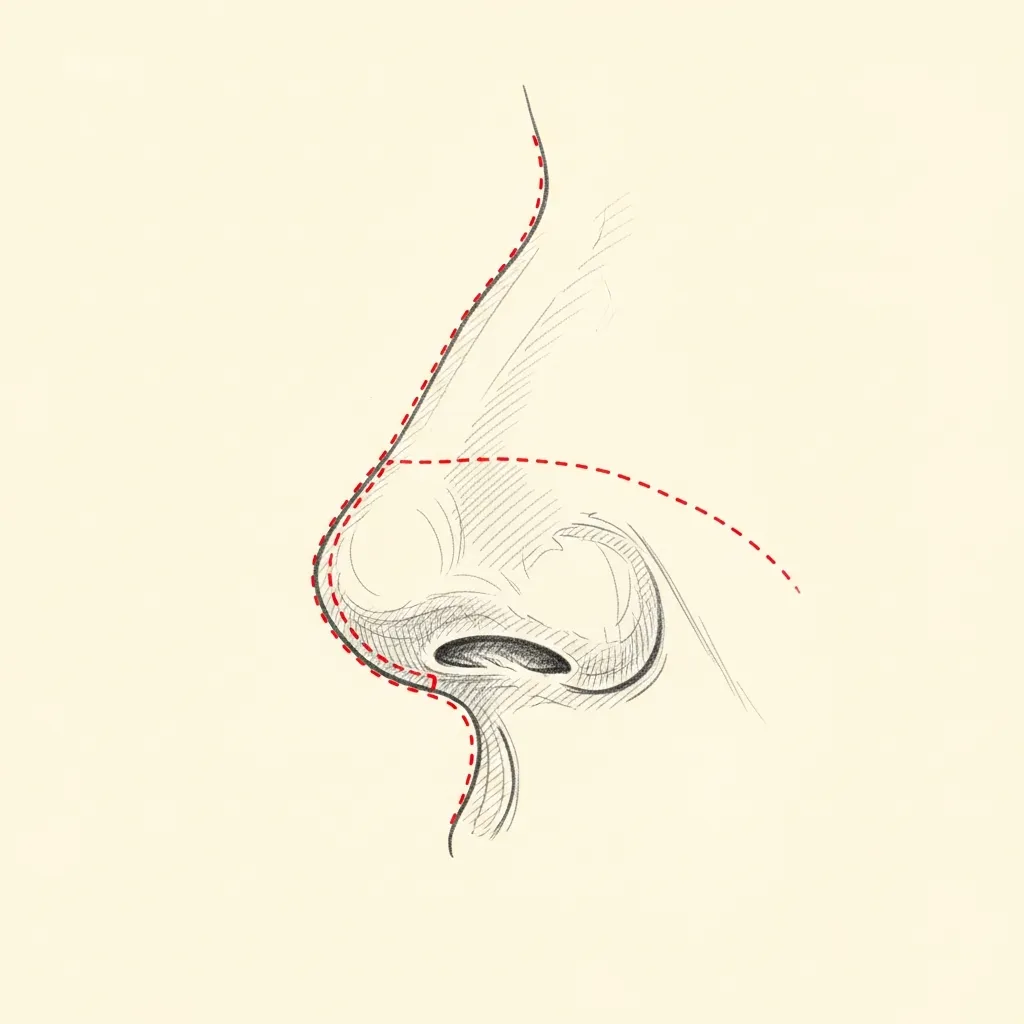
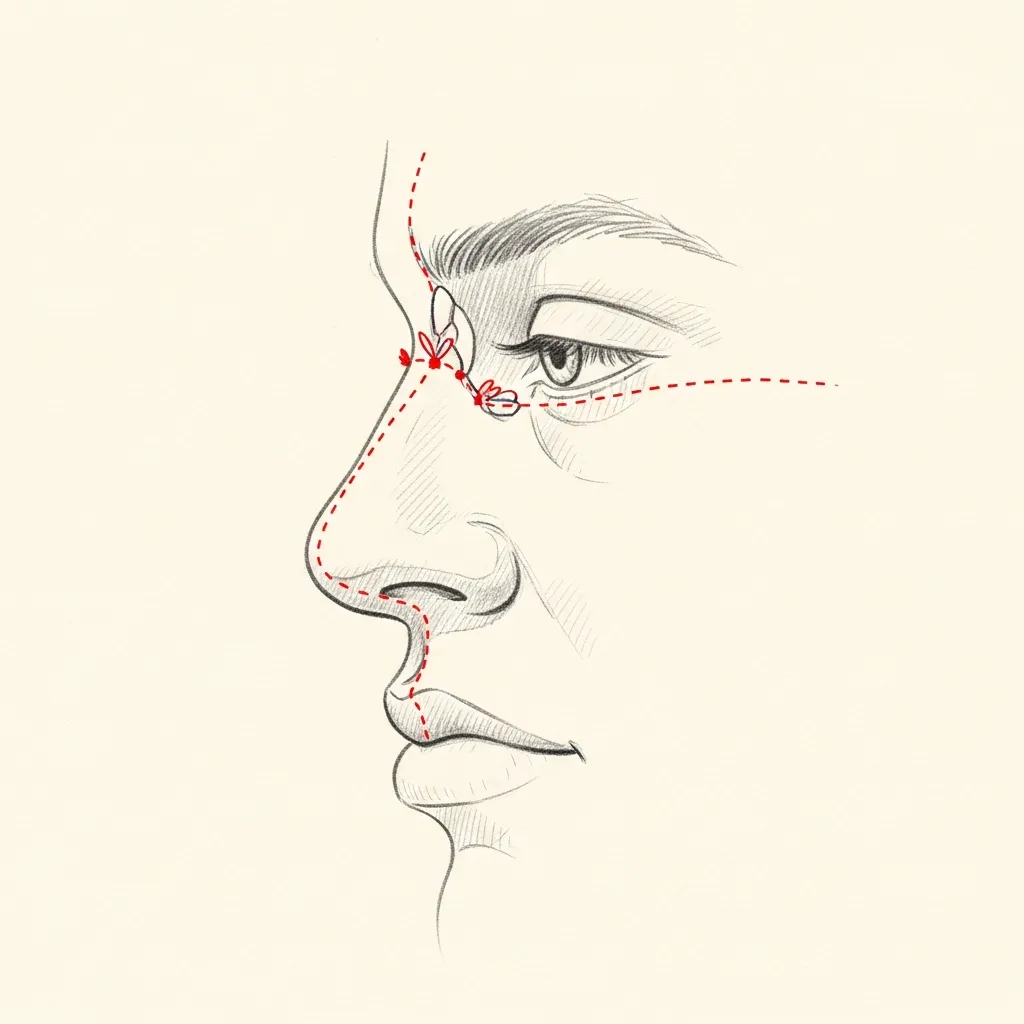
Soft-tissue vs structural pollybeak.
The treatment differs entirely. The first job at consultation is to determine which type is present.
Soft-Tissue
Often responds to non-surgical management
Soft-tissue pollybeak results from accumulated scar tissue and oedema in the supratip area after rhinoplasty. It often improves with time and may respond to taping and selective steroid injection.
This is the more forgiving form and the right one to recognise before recommending revision surgery.
Structural
Requires revision rhinoplasty
Structural pollybeak occurs when the dorsal cartilage is not adequately reduced relative to the tip — or when the tip itself is under-projected. The bony or cartilaginous excess is visible and palpable.
Correction requires revision rhinoplasty — either reducing the supratip cartilage, increasing tip projection, or both. Revision is generally deferred at least 12 months after the prior operation.
Illustrative diagrams. The right management depends on which type of pollybeak is present.
04 · Diagnosis
How the diagnosis is made.
Diagnosis is clinical, made on examination and lateral profile photography.
The distinction between soft-tissue pollybeak (scar-tissue accumulation) and structural pollybeak (cartilage or bony excess) is the key diagnostic question.
Photographs from before and after prior surgery, when available, clarify whether the deformity is new or pre-existing.
05 · Treatment Options
Treatments matched to the diagnosis.
Treatment is individual. The right answer ranges from optimised medical therapy to a focused procedure to definitive surgery.
Non-Surgical Management
Steroid injection and taping for soft-tissue pollybeak in selected post-rhinoplasty patients.
Learn More
Revision Rhinoplasty
Structural correction for cartilage or bony pollybeak — typically requires 12 months after the prior surgery.
Learn More
Tip Refinement
Often combined with pollybeak correction — improving tip projection is part of restoring the supratip-tip relationship.
Learn More
01 · Why Dr. Mourad
Diagnosis first, treatment second.
Dr. Mourad specialises in revision rhinoplasty and evaluates pollybeak deformity for both its soft-tissue and structural components.
A careful examination distinguishes scar-tissue pollybeak (which often responds to non-surgical management) from structural pollybeak (which requires revision surgery).
When revision is required, it is approached with the same restraint as a primary operation — the cause is corrected, no more.
When to Seek Care
When to seek care promptly.
New significant nasal asymmetry or fullness shortly after surgery — contact your surgeon.
Persistent severe pain weeks after rhinoplasty — evaluate promptly.
Sudden change in nasal shape after trauma to an operated nose — evaluate immediately.
Signs of infection (warmth, redness, drainage) after recent surgery — evaluate urgently.
Outlook
What to expect.
When the diagnosis is correct and the right treatment is applied, the outlook is generally good. Most patients describe meaningful improvement in symptoms and day-to-day function.
When symptoms persist despite treatment, the workup is re-opened. Persistent symptoms with no answer almost always mean the diagnosis is incomplete.

Living Well
Day-to-day measures that help.
Daily saline irrigation, control of indoor allergens, and good sleep hygiene meaningfully reduce day-to-day symptoms for many patients.
Medical therapy, when prescribed, works best when used consistently rather than as needed — this is one of the most common reasons treatment seems to fail.
Frequently Asked
Patient questions, honestly answered.
A pollybeak deformity is a convex supratip prominence seen on the lateral profile, producing a beak‑like silhouette above the nasal tip. Identification requires static and dynamic profile photographs and a physical exam of tip support. The surgeon differentiates soft‑tissue bulk from residual dorsal cartilage and tip ptosis. That distinction directs whether revision will focus on scar release, dorsal contouring, or structural support.
Post‑operative pollybeak commonly results from multiple interacting factors rather than a single error. Residual dorsal cartilage or intentionally preserved dorsal height can appear excessive if the tip subsequently loses support. Subcutaneous scar, skin envelope thickness, and tip ptosis from weakened support also magnify a supratip fullness. A careful review of prior operative notes, photographs, and the soft‑tissue response helps identify the dominant cause.
Definitive revision is typically planned after tissue maturation, usually around 12 months post‑op when most swelling has resolved. In patients with very thick skin or prolonged edema, improvement may continue and planning can extend to 12–18 months. Early clinic assessments are reasonable to document the issue and discuss timing, but definitive structural revision is rarely advisable before maturation. Exceptions are made for acute functional problems and are handled case‑by‑case.
Non‑surgical measures are limited and mainly temporizing for mild supratip scarring or edema. Selective intralesional corticosteroid injections can soften focal scar contracture and reduce localized thickness over several sessions. Injectables that add volume are generally contraindicated because they worsen prominence. Skin‑directed treatments such as resurfacing may improve texture but will not correct residual cartilage or structural support problems.
Surgical correction targets the specific anatomic contributors identified at evaluation. Techniques include direct dorsal contouring or rasping, subcutaneous scar release with conservative thinning, and restoration of tip support using sutures or structural grafts. An open approach is often preferred in revision to permit careful scar release and precise graft placement. Intraoperative findings frequently refine the plan, and staged procedures are sometimes safer for heavily scarred noses.
Cartilage grafting is indicated when native support is insufficient or prior harvests have depleted local sources. Septal cartilage is preferred when available and intact; auricular cartilage suits moderate reconstruction with curved segments. Costal (rib) cartilage is reserved for larger reconstructive needs or when septal and auricular tissue are unavailable. Choice depends on the degree of support required, prior operations, and the patient’s anatomic needs.
Dense subcutaneous scarring tethers the supratip and prevents natural redraping after contour work, often necessitating direct scar release or adhesiolysis. Scar management reduces bulk but increases the risk of prolonged swelling and delayed contour maturation. Patients with a high tendency to form hypertrophic scars may need staged interventions and adjunctive measures. Honest discussion about predictability and the possible need for secondary procedures improves decision making.
Yes; many patients with post‑rhinoplasty contour issues also have functional contributors such as septal deviation or internal valve narrowing. A combined septorhinoplasty approach permits simultaneous contour refinement and targeted airway procedures like septoplasty, turbinate reduction, or valve grafting. Functional assessment with anterior rhinoscopy and, when indicated, endoscopy is part of the preoperative evaluation. Addressing both form and function in a single plan often produces more durable results.
Patients with uncontrolled medical comorbidities or active infection are not suitable candidates until conditions are optimized. Active nicotine use, poorly controlled diabetes, unstable cardiac or pulmonary disease, and untreated skin breakdown or infection must be addressed before elective revision. Individuals with untreated body‑image disorder or unrealistic expectations warrant psychological evaluation prior to surgery. When septal and auricular donor tissue are exhausted and the patient refuses costal grafting, durable reconstruction may not be possible; optimization steps include smoking cessation, medical clearance, and, if needed, psychiatric referral.
Days 0–3: expect moderate swelling and mild pain controlled with oral medication; keep head elevated and follow splint and wound care instructions. Week 1: splint and most external dressings are typically removed; bruising and sharp swelling decrease; avoid bending and heavy lifting. Weeks 2–4: visible bruising usually resolves; return to desk work is common; gentle cardio may resume with surgeon approval. Weeks 4–8: swelling continues to fall, but subtle contour changes persist; resume more strenuous activity per surgeon guidance. Months 3–6: majority of soft‑tissue settling occurs and improvements become clearer. Months 6–12 and 12–18: refinement continues and final contour often matures by 12–18 months. Contact the surgeon urgently for fever, increasing pain, or sudden asymmetry.
Choose a surgeon with focused experience in revision rhinoplasty and a demonstrable approach to structural problems and scar management. During consultation, ask about their evaluation process, grafting philosophy, and experience with costal cartilage when needed. Request to review case examples and ask how they assess both form and airway function. A measured plan, clear discussion of risks, and a willingness to stage complex cases are indicators of appropriate surgical judgment.
The Most Important Step
Get an expert evaluation.
A careful evaluation by a double board-certified physician is the right first step. The conversation is unhurried, the diagnosis is honest, and treatment is matched to what you actually have.