Double Board Certified · Minimally Invasive Facelift
Endoscopic Mid-Face Lift — minimally invasive, anatomically honest.
Endoscopic mid-face lifting is a real, technique-defined operation: small incisions inside the hairline and mouth, an endoscope, and precise repositioning…
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"The word "incisionless" gets misused. A truly incisionless lift does not exist. What exists are very small, very well-hidden incisions — and an honest conversation about what each technique can and cannot do."
Before & After
Facelift results from the practice.

Facelift + Neck Lift · 50s · Female

Facelift · 50s · Female

Facelift + Neck Lift + Blepharoplasty · 50s · Female

Facelift + Neck Lift + Rhinoplasty · 50s · Female

Facelift + Neck Lift · 60s · Male

Revision Facelift + Neck Lift · 70s · Female
Pre and post-operative comparison · Photographed in standardized studio conditions · Written consent on file · Individual results vary
A Note from Dr. Mourad
"Endoscopic mid-face lifting is a real, technique-defined operation: small incisions inside the hairline and mouth, an endoscope, and precise repositioning of the mid-face tissues. It is not a substitute for a full facelift, and it is not for every patient."
— Dr. Moustafa Mourad, MD
Overview
What is an endoscopic mid-face lift?
An endoscopic mid-face lift is a minimally invasive surgical procedure that repositions the soft tissues of the cheek and lower eyelid through small incisions hidden inside the hairline and the mouth, with the operation guided by a small camera (endoscope). There are no visible facial incisions.
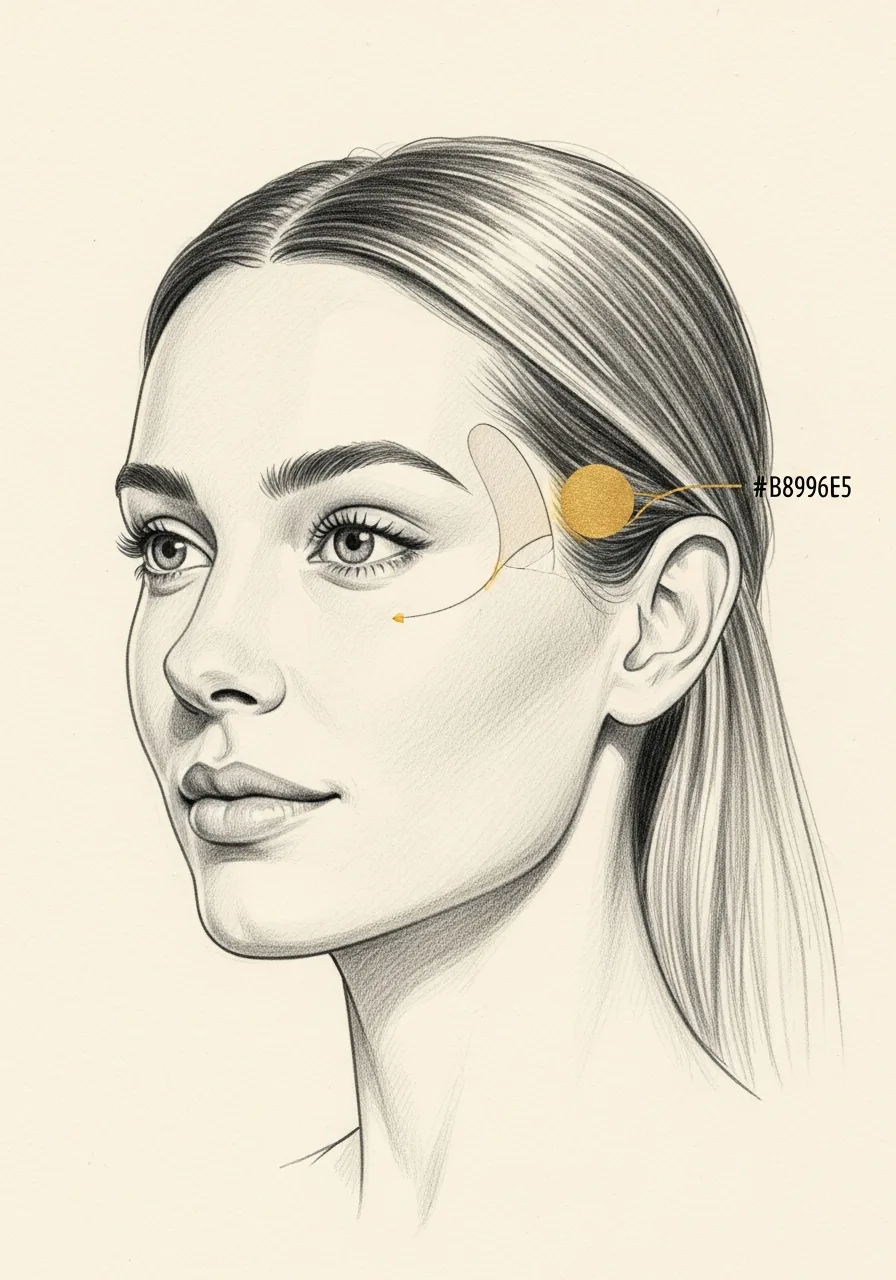
It addresses the descent of the mid-face that produces flat or hollow cheeks, a deepened nasolabial fold, a lengthened lower eyelid, and a tired appearance to the eyes. The cheek pad is lifted vertically and resuspended to its original anatomic position rather than pulled obliquely.
The endoscopic approach is well suited to younger patients with early mid-face descent who do not yet need a full lower facelift, and to selected patients who want to avoid pre-auricular incisions. It is not a substitute for a lower facelift when the jowls and neck are the primary concern.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
01 · Why Dr. Mourad
Diagnosis first, then a plan that fits.
Dr. Mourad does not market techniques that do not exist. The endoscopic mid-face lift is offered when it is the right answer — not when a flashy name will sell.
Patient selection is rigorous: the right candidate has mid-face descent without significant neck or jawline change.
When fuller facial rejuvenation is needed, a deep-plane facelift is recommended candidly — even when the patient came in asking for the smaller operation.
02 · Ideal Candidates
Who benefits most from this operation.
Candidacy is determined together at consultation. The most satisfied patients share three things in common.
I
Isolated Mid-Face Descent
Patients in their forties or early fifties with descent of the cheek and mid-face but a still-defined jawline and neck.
II
Early Aging Anatomy
Patients seeking modest, natural-looking rejuvenation through a smaller operation with a shorter recovery.
III
Honest Expectations
Patients who understand this is a smaller operation than a deep-plane facelift, with a smaller — and earlier — result.
Before & After
Endoscopic Facelift Before and After Cases
Documented facelift and neck lift results from the Manhattan practice, photographed in standardized studio conditions with written consent on file. The endoscopic mid-face approach suits selected patients with brow and midface concerns; the right approach is determined at consultation. Individual results vary with anatomy and goals.

Facelift + Neck Lift · 50s · Female
Facelift combined with a neck lift for a female patient in her 50s to address midface and jawline laxity along with submental and neck fullness. Documented in frontal, oblique, and lateral views before and after surgery; photographed in standardized studio conditions with written consent on file.

Facelift + Neck Lift · 60s · Male
Facelift combined with a neck lift for a male patient in his 60s to address midface, jawline, and neck laxity. Documented in oblique and lateral views before and after surgery; photographed in standardized studio conditions with written consent on file.
Pre and post-operative comparison · Photographed in standardized studio conditions · Written consent on file
If this describes you, the next step is a quiet, unhurried conversation — not a sales call.
An Honest Note
When this operation may not be right for you.
Patients with significant jowling, neck banding, or platysmal laxity will not get a satisfactory result from a mid-face-only operation.
Patients seeking the result of a deep-plane facelift through a smaller operation will be disappointed.
Patients in their sixties and beyond with multi-zone aging are typically better served by a comprehensive lift.
Patients whose concerns are primarily skin texture or pigment, not laxity, benefit from a non-surgical resurfacing plan first.
03 · Approaches
Three paths to mid-face rejuvenation.
The endoscopic mid-face lift is an early-intervention option. The right plan depends on whether the rest of the face has aged in parallel, or whether the mid-face is genuinely the only concern.
1 of 3 · Endoscopic Mid-Face Lift
04 · Technique
Endoscopic vs deep-plane facelift.
Two very different operations addressing different anatomic problems. The choice between them is the most important conversation at consultation.
Endoscopic
Mid-face only, smaller recovery
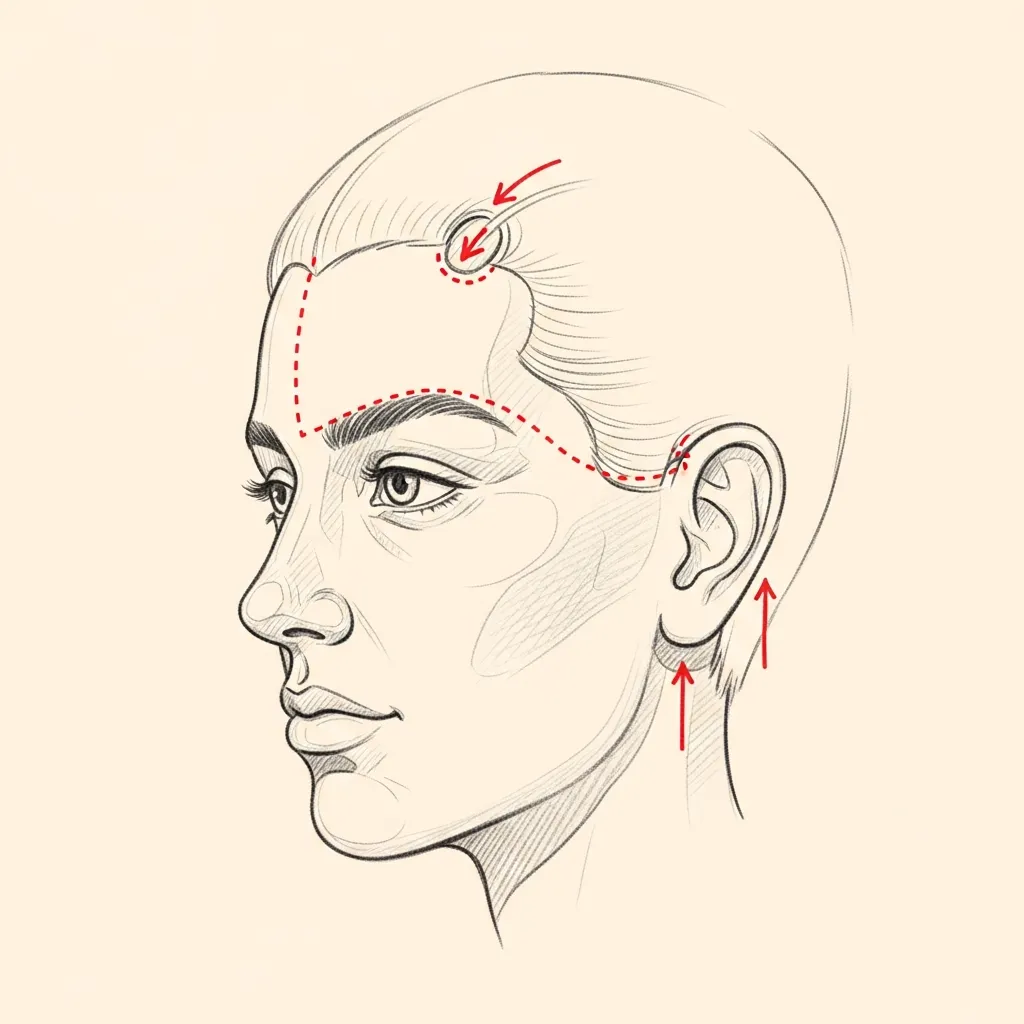
Two small incisions are made inside the temporal hairline and one inside the mouth. An endoscope visualises the deeper tissues and the malar fat pad is repositioned vertically.
Recovery is shorter than a full facelift — typically one week of meaningful downtime — and the scars are essentially invisible. The result is real but limited to the mid-face.
Deep-Plane
Comprehensive mid-face, jawline, neck
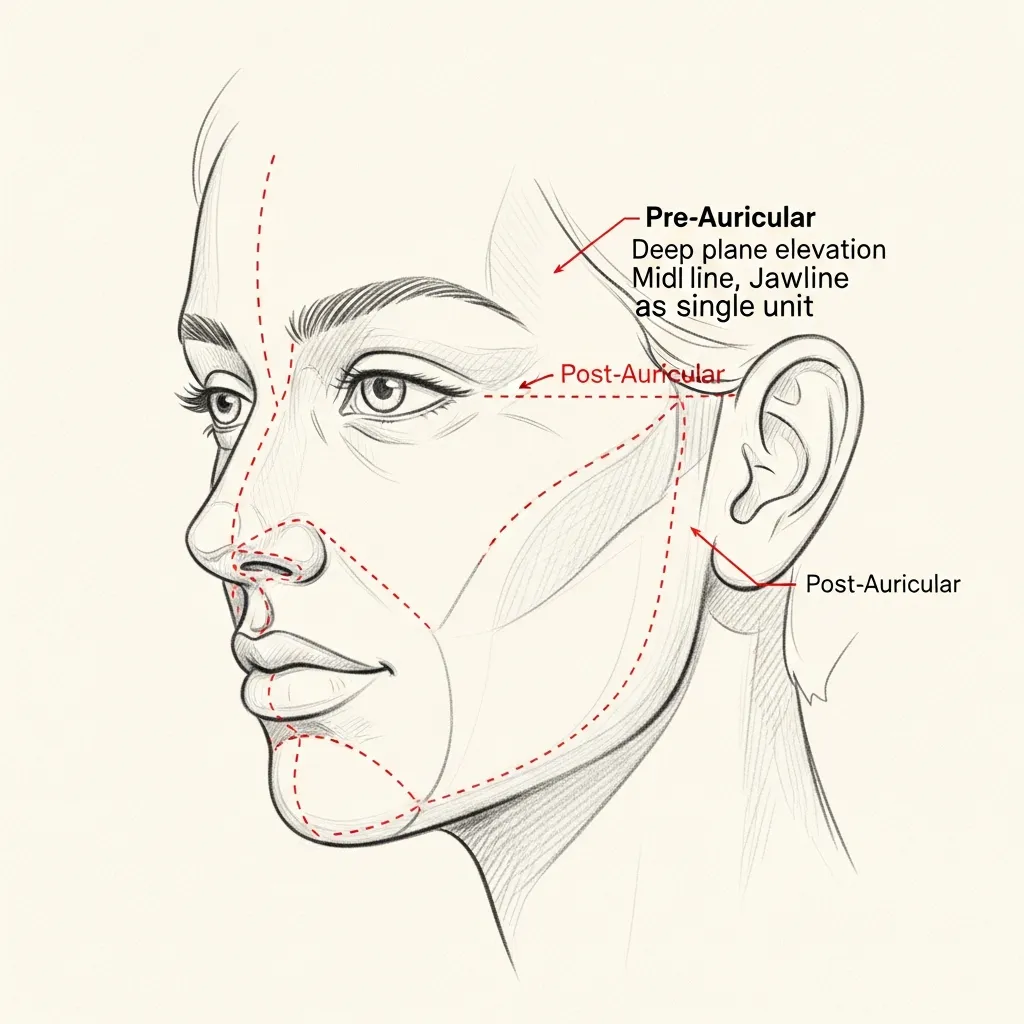
A deep-plane facelift addresses the mid-face, jawline, and neck through pre- and post-auricular incisions hidden along the ear. It produces a far more comprehensive — and durable — result.
When the anatomy calls for it, a deep-plane lift is the right operation. A smaller operation in the wrong patient is not a kindness.
Illustrative diagrams. The right operation is determined by the anatomy presented at consultation.
Begin the conversation
A careful, honest evaluation is the right first step.
Cost, Financing & Insurance
Endoscopic Mid-Face Lift Cost, Financing & Insurance in NYC
The cost of an endoscopic mid-face lift depends on the areas being treated, the extent of lifting required, whether it is combined with other facial procedures, the type of anesthesia, and the surgical setting. Each plan is individualized after facial evaluation.
This procedure is generally considered cosmetic and is typically self-pay. After consultation, our office provides a personalized estimate based on the recommended plan. Financing may be available for qualified patients through third-party healthcare financing providers.
What May Affect Cost
- Areas being treated
- Extent of lifting required
- Whether combined with other procedures
- Type of anesthesia
- Surgical setting
- Postoperative care
This information is educational and is not a guarantee of pricing, insurance coverage, reimbursement, financing approval, or surgical candidacy. A personalized estimate is provided after consultation. Insurance coverage depends on the patient’s plan, medical necessity, documentation, and carrier requirements. Financing terms are determined by third-party financing providers.
06 · Recovery
What healing actually looks like.
Stage 01
First 24 Hours
Initial recovery focuses on rest, hydration, and following all post-operative instructions exactly. Pain is managed with multi-modal non-narcotic protocols where appropriate.
Stage 02
Week 1
Swelling and bruising peak in the first few days and improve steadily through the first week. Most patients are presentable for casual social activity by the end of week two.
Stage 03
Weeks 2 – 4
Through weeks two to four the early result begins to settle. Light cardio resumes around three weeks; vigorous exertion and contact activities are deferred per the operative plan.
Stage 04
Months 1 – 6
The final refined result emerges progressively over the following months as residual swelling continues to resolve. Follow-up visits are scheduled across the first year.
Have a specific question?
Send a brief note describing your anatomy or concerns — the office will route it directly to Dr. Mourad for review.

Before You Arrive
Your consultation, prepared.
Bring photographs relevant to your concern, when available.
Bring records from any prior surgery, when available.
List current medications, supplements, and blood-thinning agents.
Note any prior anesthesia issues or chronic medical conditions.
Allow 60 minutes for the first consultation.
Bring questions; no decisions are made at the first visit.
Frequently Asked
Patient questions, honestly answered.
An endoscopic mid‑face lift is a camera‑assisted surgical approach that targets descent of malar soft tissues, the mid‑face SMAS, and retaining ligaments. It primarily improves cheek projection and reduces nasolabial prominence rather than treating marked neck laxity. Access is through small hairline or temporal incisions that allow subcutaneous or sub‑SMAS release under direct visualization. The operative plan is individualized based on bony support, fat distribution, and skin quality determined at consultation.
The endoscopic technique emphasizes targeted release and internal fixation through limited incisions with less skin undermining. Deep‑plane and SMAS facelifts mobilize broader tissue segments and typically address lower face and neck laxity more comprehensively. Endoscopic lifts can be less disruptive to the skin envelope but are limited when excess neck skin or pronounced platysmal banding exists. Choice of technique is based on the specific anatomic problems identified in the clinic.
Good candidates usually have mid‑face descent with preserved skin elasticity, adequate cheek bone support, and minimal lower‑face or neck laxity. Active smoking, uncontrolled medical problems, very thin or scarred skin, and prior extensive facial surgery may reduce suitability for a limited approach. Patients seeking isolated cheek elevation or correction of early nasolabial deepening are commonly considered. Final candidacy requires clinical examination, standardized photography, and discussion of realistic objectives at an in‑person visit.
Incisions are typically placed within the hairline or temporal scalp and are small—often a few millimeters to a couple of centimeters. Because incisions sit in hair‑bearing skin, visible scars are usually minimal when wounds heal normally and hair coverage is present. Layered closure, avoidance of tension, and postoperative wound care reduce scar widening and local hair loss. Scar appearance is reviewed during preoperative counseling and monitored during follow‑up.
Endoscopic mid‑face lifts are performed in an accredited operating room under general anesthesia or deep monitored sedation, depending on extent and any concurrent procedures. Isolated cases commonly require approximately 90–180 minutes of operating time. When combined with blepharoplasty, neck work, or grafts, total time increases accordingly. Anesthesia choice and timing are planned in advance and discussed at the preoperative visit.
Expect moderate swelling and bruising that typically peaks in the first 48–72 hours and then begins to improve. Pain is generally mild to moderate and controllable with oral medications; severe pain is uncommon and should prompt contact with the surgical team. Patients often take 7–14 days off work depending on their tolerance for visible changes and job demands. Early follow‑up focuses on incision checks, dressing removal, and guidance for gradual activity progression.
Early contour changes appear as swelling subsides, often by 4–6 weeks, but soft‑tissue settling and scar maturation continue for 3–6 months. Durability depends on intrinsic skin quality, degree of fixation, age, and ongoing sun and lifestyle exposure. Fixation to deep anatomic points generally prolongs effect compared with skin‑only lifts. Maintenance options such as structural fillers or skin treatments can be discussed if desired.
Expected effects include temporary numbness, swelling, bruising, and transient asymmetry as tissues settle. Less common problems include wound healing delay, hairline thinning, infection, contour irregularities, or hematoma; each has established management pathways ranging from local wound care to minor revision or urgent evacuation in rare cases. Hematoma is uncommon but recognized and treated promptly when present. All risks and contingency plans are reviewed during informed consent.
Yes. Combining an endoscopic mid‑face lift with upper or lower blepharoplasty or selective neck procedures is common when the exam indicates multi‑region aging. The decision to combine operations balances increased operative time, anesthesia plan, and recovery expectations. When significant neck skin excess or platysmal banding is present, a separate or extended lower‑face/neck approach may be more appropriate. These tradeoffs are discussed and recorded during preoperative planning.
Alternatives include deep‑plane or SMAS facelifts for more extensive laxity, targeted neck‑lift procedures for platysmal changes, or non‑surgical options such as dermal fillers and skin‑directed therapies for volume and texture. Thread lifts and filler strategies can provide temporary improvement but have different durability and indications. The right option depends on the anatomic problem and patient priorities. Dr. Mourad reviews these choices and expected recovery during consultation.
The Most Important Step
Your expert consultation.
A careful evaluation by a double board-certified physician is the right first step. The conversation is unhurried, the diagnosis is honest, and the operative plan is built around what your anatomy can sustain and what you actually want.