Double Board Certified · Functional Sinus Care
Odontogenic Sinusitis — when the cause is dental, the cure is too.
Odontogenic sinusitis is sinus inflammation caused by dental infection or dental procedure. It accounts for a meaningful share of unilateral maxillary…
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"Maxillary sinusitis that does not respond to standard treatment frequently has a dental cause that has been overlooked."
A Note from Dr. Mourad
"Odontogenic sinusitis is sinus inflammation caused by dental infection or dental procedure. It accounts for a meaningful share of unilateral maxillary sinusitis and is consistently under-diagnosed — because the dental and sinus evaluations are usually done by different specialists."
— Dr. Moustafa Mourad, MD
Overview
What is odontogenic sinusitis?
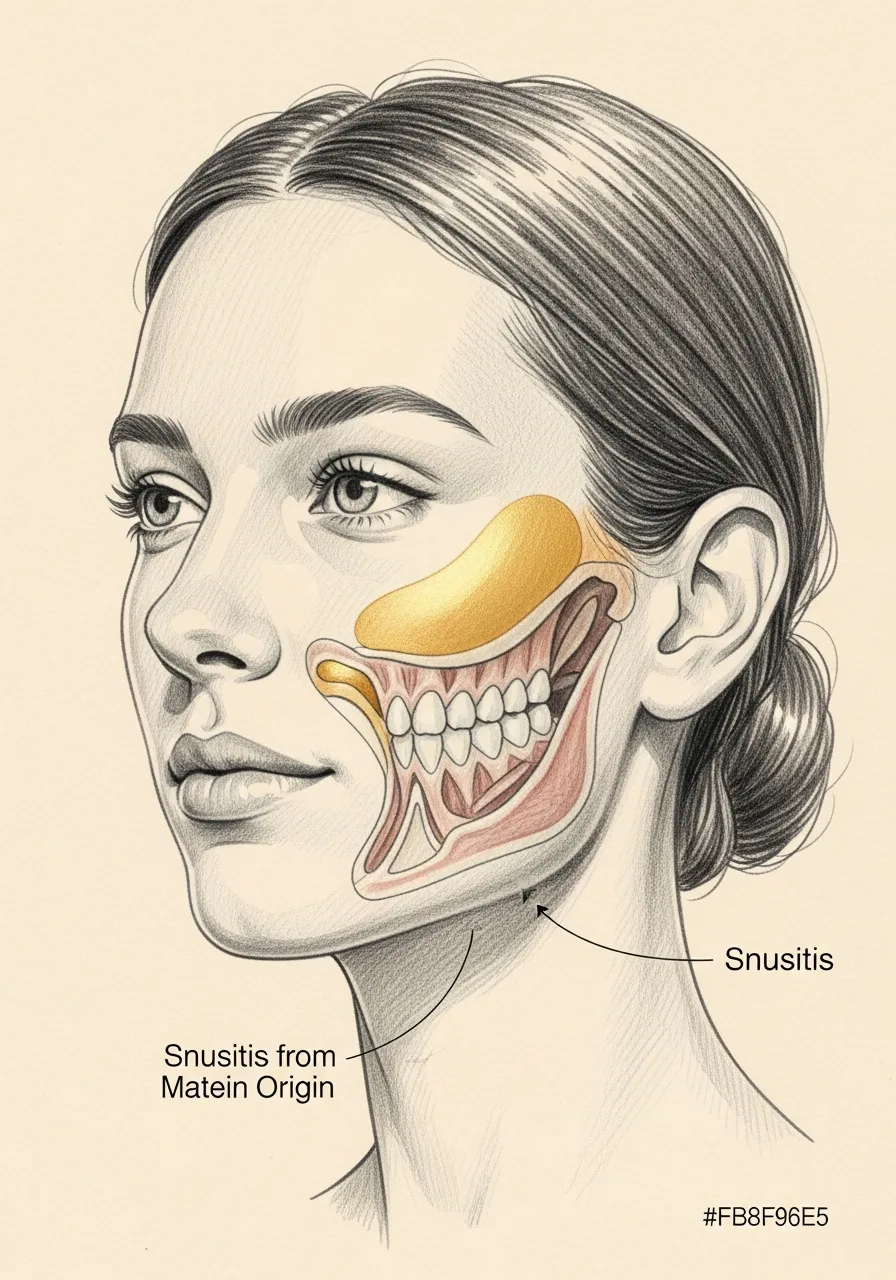
Odontogenic sinusitis is sinus inflammation caused by a dental source — most commonly an infected upper molar or premolar, a periapical abscess, a failed root canal, or a complication of dental implant or extraction. Because the roots of the upper back teeth sit immediately below the floor of the maxillary sinus, dental disease can extend into the sinus and produce chronic, often one-sided sinusitis.
It is frequently missed because the patient and the treating physician focus on sinus symptoms while the underlying dental cause goes unaddressed. Recurrent unilateral maxillary sinusitis, foul-smelling discharge, or sinusitis that does not respond to standard treatment should raise suspicion for a dental source.
Accurate diagnosis requires coordinated evaluation — nasal endoscopy plus imaging that includes the dental roots (CT or CBCT). Treatment is twofold: the dental source must be addressed by a dentist, oral surgeon, or endodontist, and persistent sinus disease is treated medically or surgically as appropriate.
Key takeaways
- Odontogenic sinusitis is sinus inflammation from a dental source — "odontogenic" means tooth-origin.
- Upper molar roots sit just below the maxillary sinus floor, so dental disease can spread upward.
- It is commonly one-sided and consistently under-diagnosed.
- Foul-smelling discharge or sinusitis that resists standard treatment should raise suspicion.
- Both the dental source and the sinus must be treated; sinus surgery alone is incomplete.
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
Castle Connolly Top Doctor — Plastic Surgery, 202602 · Symptoms
How this condition typically presents.
Three patterns are most common. Patients often recognise themselves in one or more of these.
I
Unilateral Maxillary Symptoms
One-sided cheek pain, pressure, and congestion that does not respond to standard sinus treatment.
II
Foul Odour or Taste
A characteristic foul smell or taste — often the strongest clue to a dental cause.
III
Recent Dental History
Recent dental work, tooth extraction, or known untreated dental infection on the affected side.
03 · Anatomy
Dental & sinus anatomy.
The upper molar roots sit immediately beneath the floor of the maxillary sinus. The proximity is what makes odontogenic sinusitis possible.
Anatomy
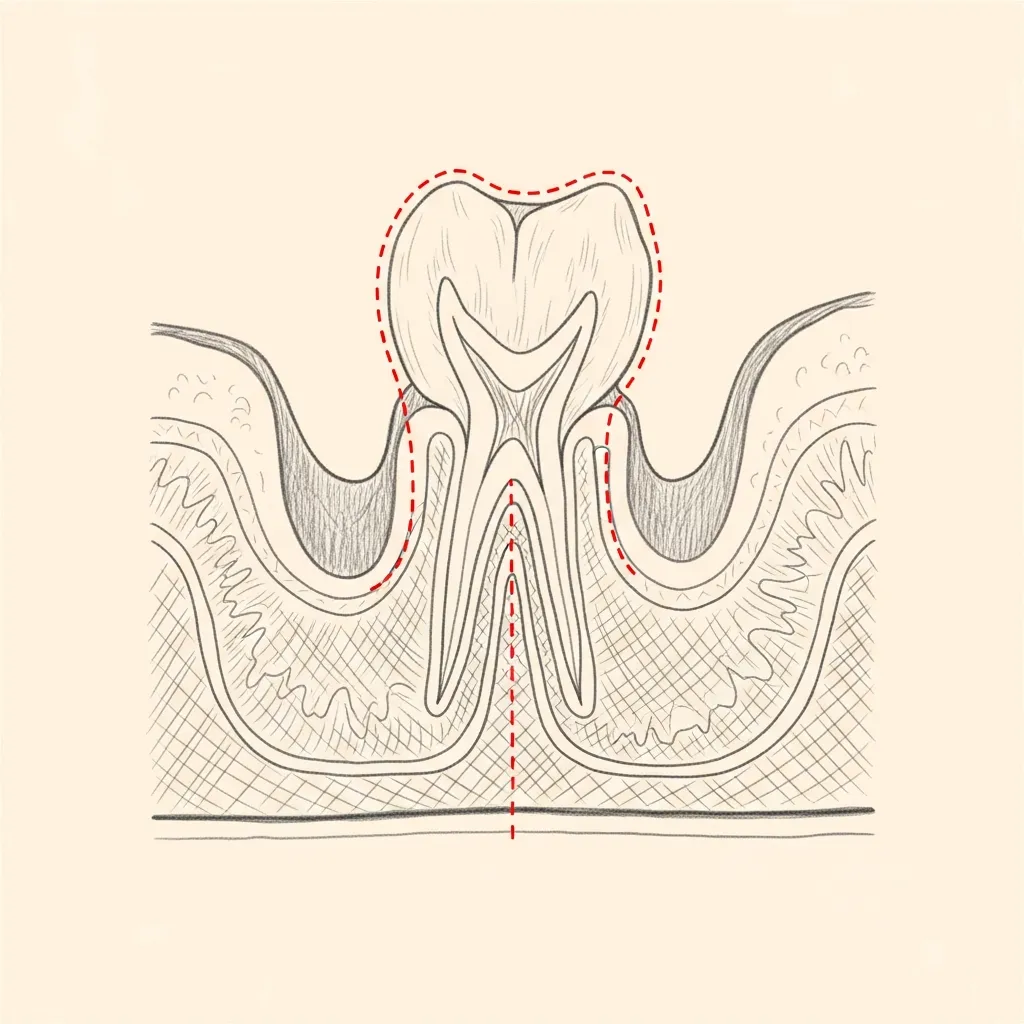
Root tips adjacent to the sinus floor
The roots of the upper molars frequently sit just below — sometimes within — the floor of the maxillary sinus. A periapical dental infection can extend directly into the sinus.
This anatomy is also why an upper tooth extraction can leave an oroantral communication — a small fistula between the mouth and the sinus.
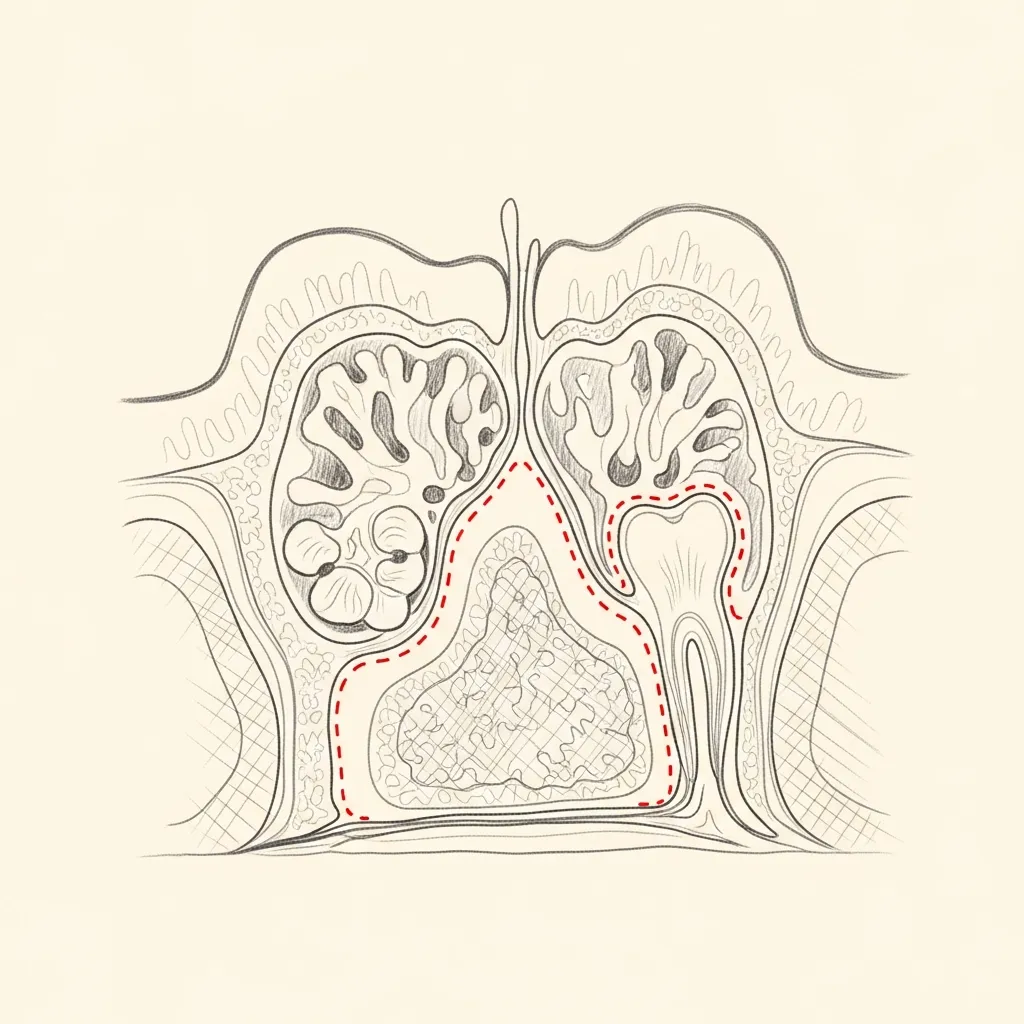
Pathology
Sinus disease from a dental source
When a dental source produces sinus disease, the imaging characteristically shows unilateral maxillary opacification with identifiable dental pathology — periapical lucency, root canal failure, or oroantral fistula.
Sinus surgery alone does not cure the disease; the dental source must be addressed by a dental specialist, and the sinus drainage restored by an otolaryngologist.
Illustrative diagrams. Coordinated dental and sinus management is essential.
04 · Diagnosis
How the diagnosis is made.
Diagnosis is made by CT imaging — characteristic findings of unilateral maxillary disease with dental-root involvement.
Dental examination and assessment by a dental specialist is essential.
Endoscopic examination confirms the sinus findings and assesses the drainage pathway.
05 · Treatment Options
Treatments matched to the diagnosis.
Treatment is individual. The right answer ranges from optimised medical therapy to a focused procedure to definitive surgery.
Dental Source Management
Treatment of the underlying dental cause — extraction, root canal, or repair of an oroantral fistula.
Learn More
Endoscopic Sinus Surgery
Drainage and clearance of the affected sinus, typically performed after or with dental management.
Learn More
Medical Therapy
Targeted antibiotics, saline irrigation, and supportive care as part of combined management.
Learn More
01 · Why Dr. Mourad
Diagnosis first, treatment second.
Dr. Mourad coordinates evaluation with dental specialists when odontogenic sinusitis is suspected — both the sinus and the source must be addressed.
CT imaging is essential to identify dental pathology and to plan combined treatment.
Sinus surgery alone — without addressing the dental source — produces incomplete and short-lived improvement.
When to Seek Care
When to seek care promptly.
Severe facial pain, swelling, or fever — evaluate within days.
Significant facial swelling or redness around the eye — evaluate immediately.
Numbness of the cheek or upper teeth — evaluate promptly.
Persistent oroantral fistula after recent dental extraction — evaluate within days.
Outlook
What to expect.
When the diagnosis is correct and the right treatment is applied, the outlook is generally good. Most patients describe meaningful improvement in symptoms and day-to-day function.
When symptoms persist despite treatment, the workup is re-opened. Persistent symptoms with no answer almost always mean the diagnosis is incomplete.

Living Well
Day-to-day measures that help.
Daily saline irrigation, control of indoor allergens, and good sleep hygiene meaningfully reduce day-to-day symptoms for many patients.
Medical therapy, when prescribed, works best when used consistently rather than as needed — this is one of the most common reasons treatment seems to fail.
Frequently Asked
Patient questions, honestly answered.
Odontogenic sinusitis is maxillary sinus inflammation driven primarily by disease of a tooth or its supporting structures. Unlike viral or allergic sinusitis, it is often strictly one‑sided and associated with dental symptoms or recent dental work. Diagnosis depends on correlating nasal endoscopy, dental exam, and imaging such as periapical films or CBCT to demonstrate a dental source. Treatment requires addressing the dental nidus as well as sinus drainage; ENT and dental specialists commonly coordinate care.
Posterior maxillary teeth (first and second molars, sometimes premolars) most frequently cause odontogenic sinusitis because their roots are nearest the sinus floor. A periapical abscess, advanced periodontal disease, or implant migration from these teeth can breach the sinus or create a chronic communication. CBCT reliably shows the spatial relationship between roots, implants, and the sinus floor, which helps determine whether the tooth is the likely source.
Red flags for an odontogenic cause include persistent unilateral purulent nasal drainage, a fetid nasal odor, focal maxillary tooth pain, or a recent history of extraction, implant placement, or root canal. On nasal endoscopy, localized purulence in the middle meatus or an oroantral communication visible intraorally increases suspicion. Because symptoms overlap with other causes, imaging and direct dental evaluation are required to confirm the diagnosis.
Initial assessment often includes periapical radiographs or a panoramic film to map dental pathology. When a dental source is suspected or surgical planning is likely, Dr. Mourad requests cone‑beam CT (CBCT) because it delineates root anatomy, sinus floor status, mucosal disease, and retained dental material. CBCT images are reviewed jointly with the treating endodontist, oral surgeon, or restorative dentist to plan sequencing of dental and sinus interventions.
Yes. Failed endodontic treatment, overfilled root canal material, displaced root fragments, and implants that penetrate the sinus can all seed chronic maxillary sinus inflammation. The mechanism may be direct contamination, persistent foreign material, or an oroantral communication that allows oral bacteria into the sinus. Management depends on whether the dental source can be corrected endodontically, requires extraction, or necessitates implant removal combined with sinus clearance.
Targeted antibiotics can be useful for short‑term infection control, especially when systemic signs are present, but they rarely definitively cure odontogenic sinusitis if the dental source remains. Procedures are required when there is a persistent nidus such as a non‑vital tooth, implant in the sinus, or an oroantral fistula. The typical sequence is source control by the dental specialist, often combined with endoscopic sinus surgery when mucosal disease, obstruction, or retained material prevents drainage.
Closure options depend on defect size, location, and tissue quality. Small communications may be managed with local advancement flaps such as buccal advancement, palatal rotation, or buccal fat pad mobilization. Large or heavily contaminated defects may be staged: first control infection, then perform definitive closure once inflammation has settled. Dr. Mourad coordinates the timing with dental rehabilitation plans to balance wound healing and future prosthetic needs.
Sinus surgery alone can improve drainage and reduce mucosal disease but will not reliably cure infection if the dental source remains untreated. When dental source control (endodontic retreatment, extraction, or implant removal) is performed but symptoms persist, endoscopic sinus surgery addresses residual mucosal disease and restores ventilation. The optimal approach is individualized and may be staged or performed on the same day when immediate source removal and sinus clearance are both required.
Coordination begins at the diagnostic stage with shared review of CBCT and clinical findings. Treatment planning may involve endodontists, oral surgeons, prosthodontists, and the ENT surgeon to sequence source control, fistula repair, and sinus surgery. Communication is essential for timing—particularly when implant removal or prosthetic plans could affect flap design and healing. Dr. Mourad routinely communicates imaging findings and operative recommendations to the treating dental team.
Seek urgent evaluation for rapidly worsening facial swelling, severe uncontrolled pain, fever, visual changes, or sudden clear fluid leaking from the nose or mouth after dental work. These signs can indicate spreading infection, orbital involvement, or flap breakdown and warrant prompt assessment. For non‑urgent persistent unilateral purulent drainage or fetid odor, schedule an expedited ENT and dental evaluation to avoid chronic complications.
Continue Reading
Related sinus care
The Most Important Step
Get an expert evaluation.
A careful evaluation by a double board-certified physician is the right first step. The conversation is unhurried, the diagnosis is honest, and treatment is matched to what you actually have.