Nose · Editorial Journal
Why Does My Nose Droop When I Smile?
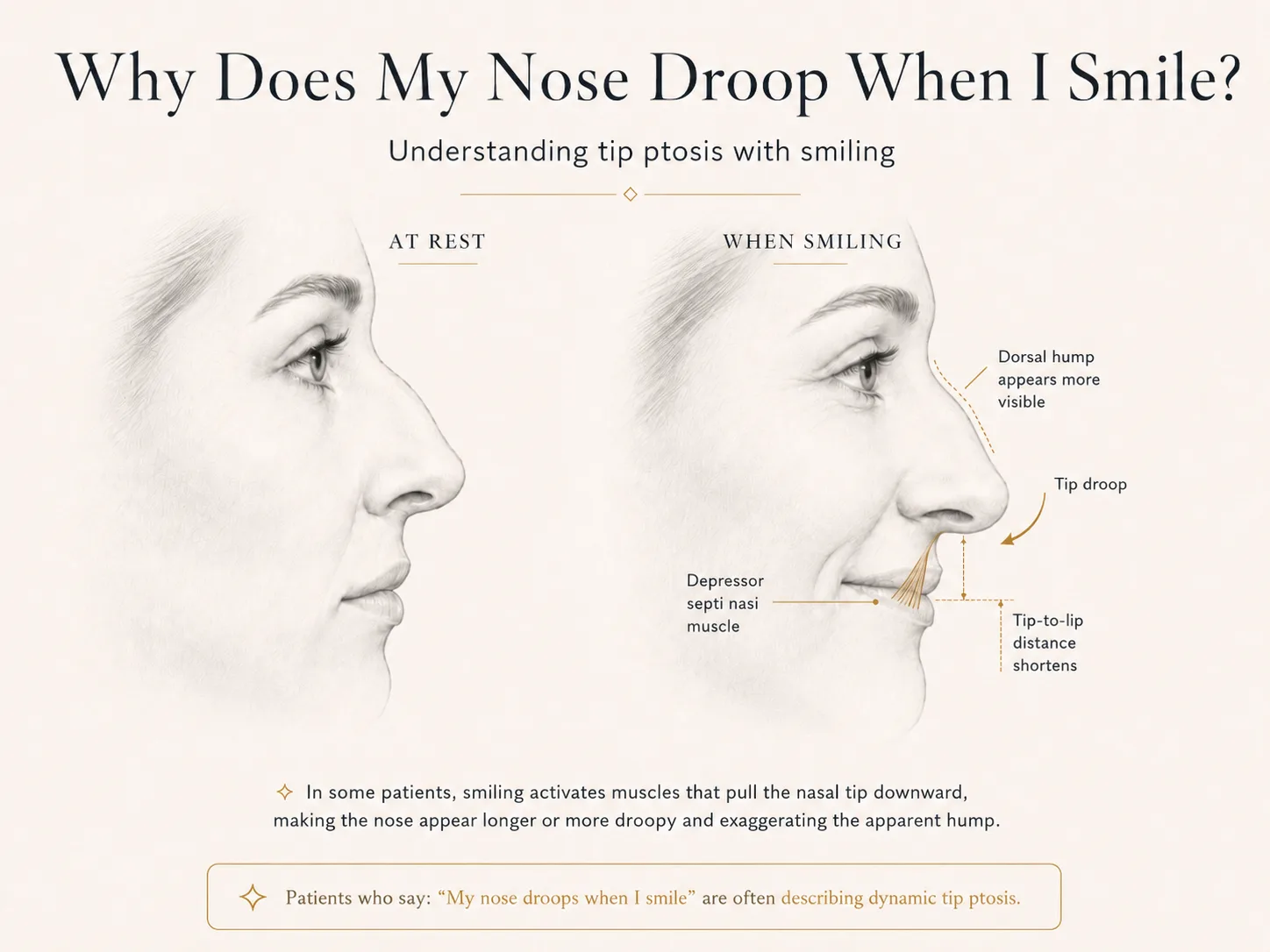
A nose that droops when smiling may reflect dynamic nasal tip ptosis. Why the tip drops with facial animation, why a hump can look more prominent, and which treatment options may help.
Many patients say some version of the same thing: “I like my nose at rest, but when I smile, the tip droops.” Others notice that the nose suddenly looks longer, the hump looks larger, or the space between the nose and upper lip seems to disappear in smiling photographs.
That change is not necessarily imagined. In some patients, smiling causes the nasal tip to rotate downward. The medical term is dynamic nasal tip ptosis: “dynamic” because it happens with facial movement, and “ptosis” because the tip descends.
The amount of movement varies widely. For one person it is a subtle change visible only in profile photographs. For another, the tip visibly dives downward whenever the upper lip elevates. Understanding why it happens is important because the best treatment depends on whether the concern is truly isolated to tip movement or is part of a broader structural rhinoplasty issue.
What are patients actually seeing?
When a patient says, “My nose droops when I smile,” the visual complaint may include several related changes:
- The nasal tip rotates downward.
- The nose appears longer.
- The tip looks heavier or less refined.
- A dorsal hump appears more prominent.
- The tip and upper lip seem closer together.
- The smile looks crowded by the nose.
- The nose appears acceptable at rest but less balanced in candid photographs.
These changes occur together because the nose is perceived as a set of relationships. The bridge, tip, columella, upper lip, and chin all influence how the profile is read. A change in one component can make another component seem larger or smaller even though it has not physically changed.
Why does the tip move when you smile?
Smiling is not produced by a single muscle. It activates a network of muscles around the mouth, upper lip, cheeks, and base of the nose. As those muscles contract, they elevate and widen the lips and change the soft-tissue tension around the nasal base.
In selected patients, the depressor septi nasi muscle contributes to downward pull on the columella and nasal tip. The muscle's effect is not identical in every person. Some patients have very little visible movement; others have a strong downward vector that becomes obvious with a full smile.
The position and strength of the lower lateral cartilages, the length and orientation of the caudal septum, the attachments around the columella, and the quality of tip support all influence how much the tip moves. This is why two people can activate the same facial expression but experience very different changes in nasal shape.
What is the depressor septi nasi muscle?
The depressor septi nasi is a small muscle located at the base of the nose and upper lip. In practical terms, it can act as a downward pull on the nasal tip and columellar region during smiling. When its effect is strong relative to the existing tip support, the tip may rotate downward.
Patients do not usually feel the muscle contracting. They notice the result: a nose that looks different in motion than it does at rest.
The muscle is only one part of the analysis. A drooping tip can also reflect weaker cartilage support, a long or low caudal septum, the shape of the columella, soft-tissue attachments, prior surgery, or a combination of these features. A good examination should not assume that every smiling-tip problem has the same cause.
Why can the dorsal hump look larger when the tip drops?
This is one of the most useful concepts in profile analysis. A dorsal hump is not judged in isolation; it is judged in relation to the tip.
Imagine a line from the upper bridge to the nasal tip. When the tip sits at an appropriate level, the hump may appear relatively mild. If the tip rotates downward, the end point of that line drops. The bridge now looks more dominant by comparison, even though the bridge itself has not changed.
- “My hump looks worse when I smile.”
- “The nose looks more hooked in pictures.”
- “It looks like the bridge gets bigger when I grin.”
The bridge is not growing during a smile. The visual relationship is changing because the tip is moving down.
In selected patients, elevating the tip can therefore make the hump appear less noticeable without directly removing it. That distinction matters. A focused tip-lift procedure may improve the balance, but it does not physically reduce a true dorsal hump. Patients who want direct hump reduction may still need formal rhinoplasty.
Why does the nose look longer when smiling?
A low or descending tip increases the visual length of the nose. The tip moves farther downward from the nasal root, and the profile can take on a heavier or more hooked appearance.
This is often most apparent in three-quarter or profile photographs. At rest, the patient may have a reasonably balanced tip. During a full smile, the tip descends, the upper lip elevates, and the nose appears to extend farther into the lower third of the face.
The result can be especially noticeable in people with a preexisting dorsal convexity or a naturally long nose, because even a small additional downward rotation may exaggerate the overall impression.
Why does the upper lip look shorter?
When the upper lip elevates during smiling and the nasal tip or columella moves downward, the visible distance between the base of the nose and the upper lip decreases. Patients often describe this as: “My nose comes down onto my lip.” “My upper lip disappears.” “The space between my nose and lip gets too short.”
This is not necessarily a true change in lip length. It is a dynamic change in the relationship between the nose and lip. The upper lip is moving up while the tip may be moving down, so the space between them appears compressed.
Why is it often worse in photographs?
A mirror usually shows a controlled, relatively static expression. Photographs capture a fraction of a second, often during a full spontaneous smile. They may also be taken from a lower angle, with a wide-angle phone lens, or at close distance — all factors that can emphasize nasal projection and tip position.
The concern is still real, but photography can amplify it. During consultation, it is helpful to evaluate standardized still photographs and, when appropriate, video or patient-provided images that show the dynamic change.
Is a drooping tip when smiling normal?
Some degree of movement is normal. Faces are dynamic, and the nose does not remain completely fixed during expression. The clinical question is whether the movement is disproportionate, bothersome, and anatomically addressable.
Treatment is not required simply because the tip moves. It becomes a cosmetic concern when the change is significant enough that the patient consistently dislikes the nose during smiling, or when the low tip contributes to broader profile imbalance.
How is the problem evaluated?
A proper evaluation looks at the nose at rest and in motion. The surgeon considers:
- resting tip rotation
- tip projection
- the amount of downward movement with smiling
- columellar position
- caudal septal anatomy
- lower lateral cartilage support
- skin thickness
- the relationship between the tip and dorsal profile
- prior trauma or nasal surgery
- breathing symptoms
- what the patient is actually trying to change
The most important question is not simply, “Does the tip move?” It is, “What structure is driving the movement, and would correcting that movement address the patient's concern?”
Can a focused in-office nasal tip lift help?
For selected patients whose main problem is a low tip or a tip that drops with smiling, a focused office procedure may be appropriate.
Nasalift™ is an in-office nasal tip elevation procedure performed under local anesthesia. Through a small internal membranous septum incision, two to three support sutures are placed to reposition the columella at a higher point along the caudal septum. This creates controlled elevation and support of the tip without a visible external scar.
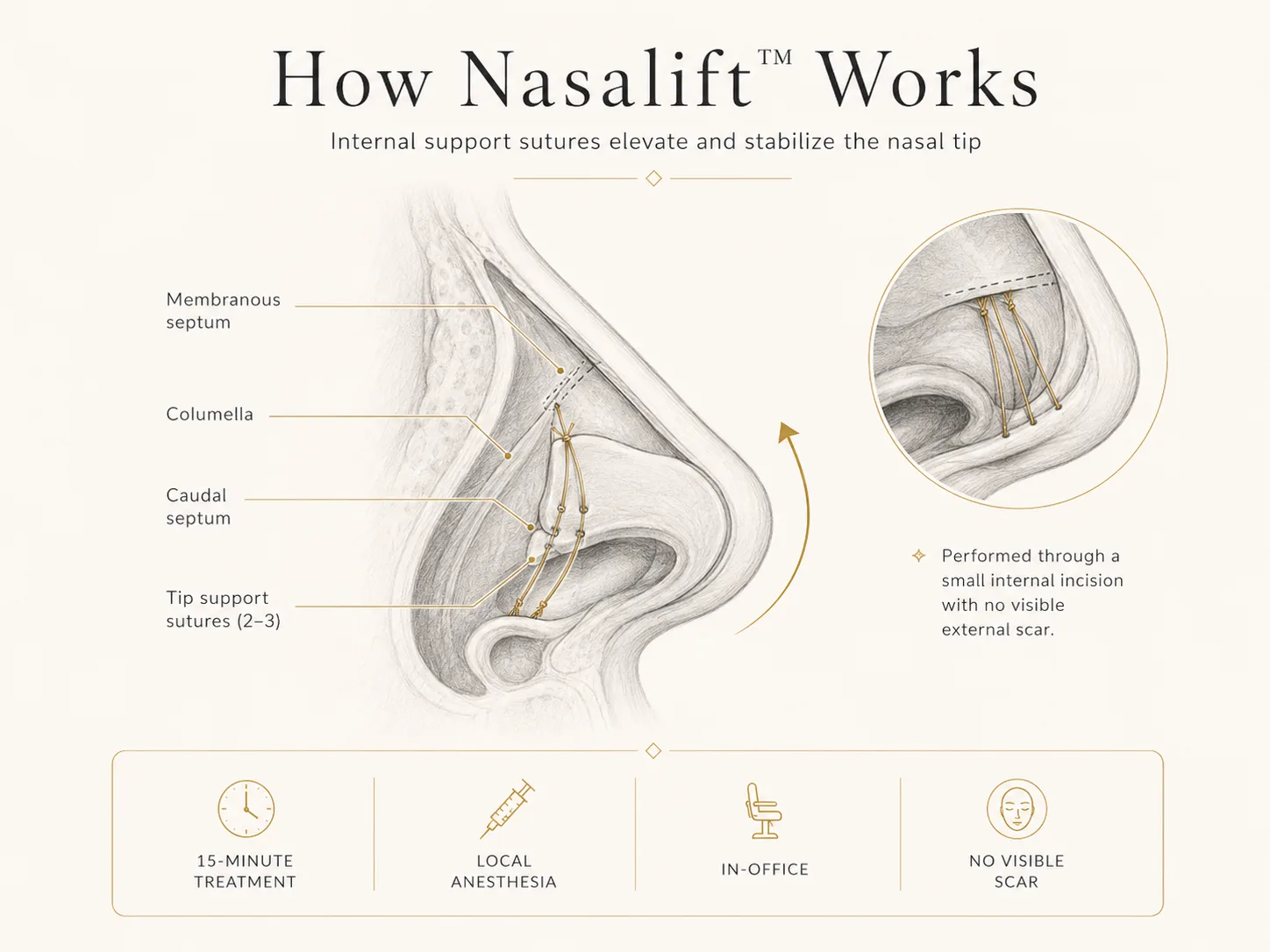
The procedure generally takes about 15 minutes. Patients typically have no bruising, minimal to no visible swelling, and little to no downtime. The aim is a subtle improvement in tip position rather than a complete reshaping of the nose.
Nasalift™ may be particularly relevant when:
- the tip is low at rest
- the tip drops further with smiling
- the nose appears longer because of tip position
- the hump appears more prominent mainly because the tip is low
- the patient wants a focused change rather than a full rhinoplasty
It is not the right treatment for every drooping tip. Anatomy and expectations determine candidacy.
When is formal rhinoplasty more appropriate?
A focused tip lift cannot address every nasal concern. Rhinoplasty may be more appropriate when the patient needs:
- direct removal or reduction of a dorsal hump
- major refinement of the tip cartilages
- narrowing of the nasal bones
- correction of substantial asymmetry
- changes in projection as well as rotation
- structural reinforcement after trauma or prior surgery
- septal or nasal valve correction for breathing
- coordinated changes across several parts of the nose
The decision should not be based only on which procedure has less downtime. It should be based on which procedure can actually accomplish the desired change safely and predictably.
Does treating the tip make the hump disappear?
No. Elevating the tip can make a hump appear less prominent by improving profile balance, but it does not remove the hump itself.
This distinction should be explained clearly. A patient with a mild hump and a low tip may be satisfied with the relative improvement created by tip elevation. A patient who wants a straight or reduced bridge may need rhinoplasty to alter the dorsum directly.
Can the problem come back?
Dynamic forces continue after any treatment. Results depend on anatomy, tissue quality, suture support, healing, and time. A focused tip-lift procedure is designed to improve support, but recurrence or partial loss of elevation may occur. This should be discussed during consultation along with the possibility of adjustment or future rhinoplasty.
Questions patients often ask
Why does only the tip move when I smile?
The amount and direction of movement depend on the balance between muscle pull and structural support. In some patients, downward muscle vectors act more noticeably on the columella-tip complex than on the rest of the nose.
Can facial exercises stop my nose from drooping?
There is no reliable facial exercise that structurally repositions a drooping nasal tip. Treatment decisions should be based on anatomy rather than internet exercise claims.
Is the hump actually getting bigger when I smile?
No. The hump itself is not enlarging. The tip is moving downward, which can make the bridge look more prominent by comparison.
Why does the space between my nose and upper lip disappear?
The upper lip elevates with smiling while the tip or columella may descend. Those opposing movements visually shorten the distance between them.
Does everyone with a drooping smiling tip need surgery?
No. Treatment is elective and depends on how much the issue bothers the patient, what anatomy is responsible, and whether a focused or comprehensive procedure is appropriate.
Can Nasalift™ replace rhinoplasty?
Only for a narrow group of patients whose primary concern is tip elevation. It cannot replace rhinoplasty when broader changes to the bridge, bones, tip cartilage, airway, or nasal framework are needed.
The key is matching the treatment to the anatomy
“My nose droops when I smile” sounds like a simple complaint, but it can reflect several overlapping relationships: muscle pull, tip support, columellar position, caudal septal anatomy, bridge height, and upper-lip movement.
The best plan begins by identifying which of those relationships is actually responsible for what the patient sees. For one patient, a focused in-office tip lift may be enough. For another, the visible tip droop may be only one part of a larger rhinoplasty problem.
A careful consultation should explain the cause, the least extensive reasonable treatment, the limitations of that treatment, and what will remain unchanged.
Continue Reading