Double Board Certified · Functional Sinus Surgery
Nasal Polyps Surgery in NYC — Precise Endoscopic Removal
Endoscopic surgery removes the polyp burden and opens the sinus drainage pathways — but polyps are an inflammatory disease, and the long-term outcome…
ABFPRS
Facial Plastic & Reconstructive Surgery
ABOto
Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
In Consultation
"Surgery is one part of polyp care. Without the medical plan that follows it, polyps return."
A Note from Dr. Mourad
"Endoscopic surgery removes the polyp burden and opens the sinus drainage pathways — but polyps are an inflammatory disease, and the long-term outcome depends as much on the medical plan after surgery as on the operation itself."
— Dr. Moustafa Mourad, MD
Medically reviewed by Moustafa Mourad, MD, FACS — dual board-certified Facial Plastic & Reconstructive Surgeon and Otolaryngologist (Head & Neck Surgery).
Last reviewed: June 2026
Start Here
This page focuses on surgery for nasal polyps
This page is for
- Endoscopic removal of nasal polyps that obstruct the airway
- Reopening the sinus drainage pathways polyps have blocked
- What the operation involves, recovery, and who is a candidate
Looking for the full picture?
- For the full range of medical and surgical treatment options, see Nasal Polyps Treatment in NYC.
Key takeaways
- Endoscopic surgery removes nasal polyps and reopens the sinus drainage pathways they have blocked.
- Polyps are an inflammatory disease, so surgery is paired with an ongoing medical plan to control recurrence.
- It is considered when symptoms persist despite optimised medical therapy like steroids and saline irrigation.
- The operation is done entirely through the nostrils with an endoscope, leaving no external incisions.
- Candidates often have airway obstruction, recurrent infections, or loss of smell from polyp burden.
Overview
What is nasal polyp surgery?
Nasal polyp surgery is an endoscopic procedure that removes nasal polyps and opens the sinus cavities they have obstructed. Polyps are soft, benign growths from chronically inflamed sinus and nasal lining; surgery addresses the obstruction and restores the access needed for long-term medical control of the underlying inflammatory disease.
It is considered when polyps are causing persistent nasal obstruction, loss of smell, recurrent infections, post-nasal drip, or facial pressure that has not responded to optimised medical therapy — typically intranasal and, when appropriate, oral steroids, saline irrigation, and biologic therapy for select patients. Surgery is rarely a stand-alone fix; it works alongside ongoing medical management.
Polyp surgery is performed entirely through the nostrils with an endoscope. There are no external incisions. The operation reopens the sinus drainage pathways and allows topical medication and saline rinses to reach the lining that drives the disease.
Meet Dr. Mourad
A nasal polyps surgeon focused on precise removal and long-term inflammation control.
Dr. Moustafa Mourad treats nasal polyps as both a surgical and an inflammatory problem. Nasal polyps can block airflow, impair smell, trap mucus, and prevent medication from reaching the sinus cavities. Surgery may be necessary when polyps obstruct the nose or sinuses, but the operation must be planned with an understanding that polyps can recur if the underlying inflammation is not controlled.
As a dual board-certified Facial Plastic and Reconstructive Surgeon and Otolaryngologist–Head and Neck Surgeon, Dr. Mourad brings both sinus-surgery and nasal-airway expertise to nasal polyps surgery in NYC. During evaluation, he reviews nasal endoscopy, CT imaging, smell changes, asthma or aspirin sensitivity when relevant, allergy history, prior steroid or antibiotic treatment, and whether balloon sinuplasty, endoscopic sinus surgery, or polyp removal is the appropriate procedure.
His philosophy is to remove obstructing disease precisely while preserving normal structures and planning for what happens after surgery. Nasal polyps surgery is not simply about clearing tissue in the operating room; it is about improving access for rinses and topical medications, restoring drainage, reducing obstruction, and setting up a long-term maintenance plan. Patients are counseled about recurrence, biologic therapy when relevant, postoperative debridement, saline irrigation, and ongoing inflammation control.
- Dual board-certified in facial plastic surgery and otolaryngology–head and neck surgery
- Endoscopic approach focused on precise removal and preservation of normal anatomy
- Long-term management philosophy for chronic inflammatory polyp disease
- Practice focused on sinus, nasal airway, facial, and reconstructive surgery
An Established Academic Authority
Double board certification. Fellowship director. Published author. A surgeon's surgeon.
ABFPRS
Board Certified
American Board of Facial Plastic & Reconstructive Surgery
ABOto
Board Certified
American Board of Otolaryngology — Head & Neck Surgery
AAFPRS
Fellowship Director
American Academy of Facial Plastic and Reconstructive Surgery
Textbook
Published Author
Contributions to the academic literature of facial plastic surgery
Dual board certification in both Facial Plastic & Reconstructive Surgery and Otolaryngology — Head & Neck Surgery.
01 · Why Dr. Mourad
Diagnosis first, then a plan that fits.
Dr. Mourad is double board-certified in Facial Plastic & Reconstructive Surgery and in Otolaryngology — a combination uniquely suited to evaluating both surgical and medical components of inflammatory sinus disease.
Every polyp surgery is paired with a medical maintenance plan — topical steroids, sometimes biologics — designed to control the underlying inflammation.
Surgery is recommended when medical therapy has been optimised and disease persists — not before.
02 · Ideal Candidates
Who benefits most from this operation.
Candidacy is determined together at consultation. The most satisfied patients share three things in common.
I
Medically-Refractory Polyps
Patients with polyps that obstruct the airway despite optimised medical therapy with topical and sometimes systemic steroids.
II
Recurrent Sinus Infections
Patients with chronic or recurrent sinus infections driven by polyp-related obstruction of the drainage pathways.
III
Loss of Smell or Quality of Life
Patients whose smell, sleep, or daily function is meaningfully reduced by polyp burden.
Illustrated Anatomy
How polyp removal restores the airway.
Nasal polyps and the surgery to remove them sit deep within the nasal cavity and sinuses — they are not visible in standard external photographs. The illustration shows polypoid tissue obstructing the middle meatus, which endoscopic surgery is designed to clear.
Illustrative anatomy · Not a patient photograph
If this describes you, the next step is a quiet, unhurried conversation — not a sales call.
An Honest Note
When this operation may not be right for you.
Patients who have not yet completed an adequate trial of topical steroid therapy benefit from medical optimisation first.
Patients whose only complaint is mild congestion without functional impact may be reasonable to manage medically.
Patients with uncontrolled asthma, aspirin sensitivity, or other systemic inflammatory disease need a coordinated plan with allergy/immunology before surgery.
Smokers should be counseled candidly about how smoking accelerates polyp recurrence.
03 · Approaches
Three paths through polyp disease.
Nasal polyps are usually a sign of underlying inflammatory disease. Surgery is one part of a longer plan that includes medical therapy and, often, biologics — the right operation depends on disease burden and what drainage is being obstructed.
1 of 3 · Endoscopic Polypectomy
04 · Technique
Polypectomy + FESS.
Polyp surgery is rarely done in isolation. The right operation usually combines polyp removal with opening of the obstructed sinus drainage pathways.
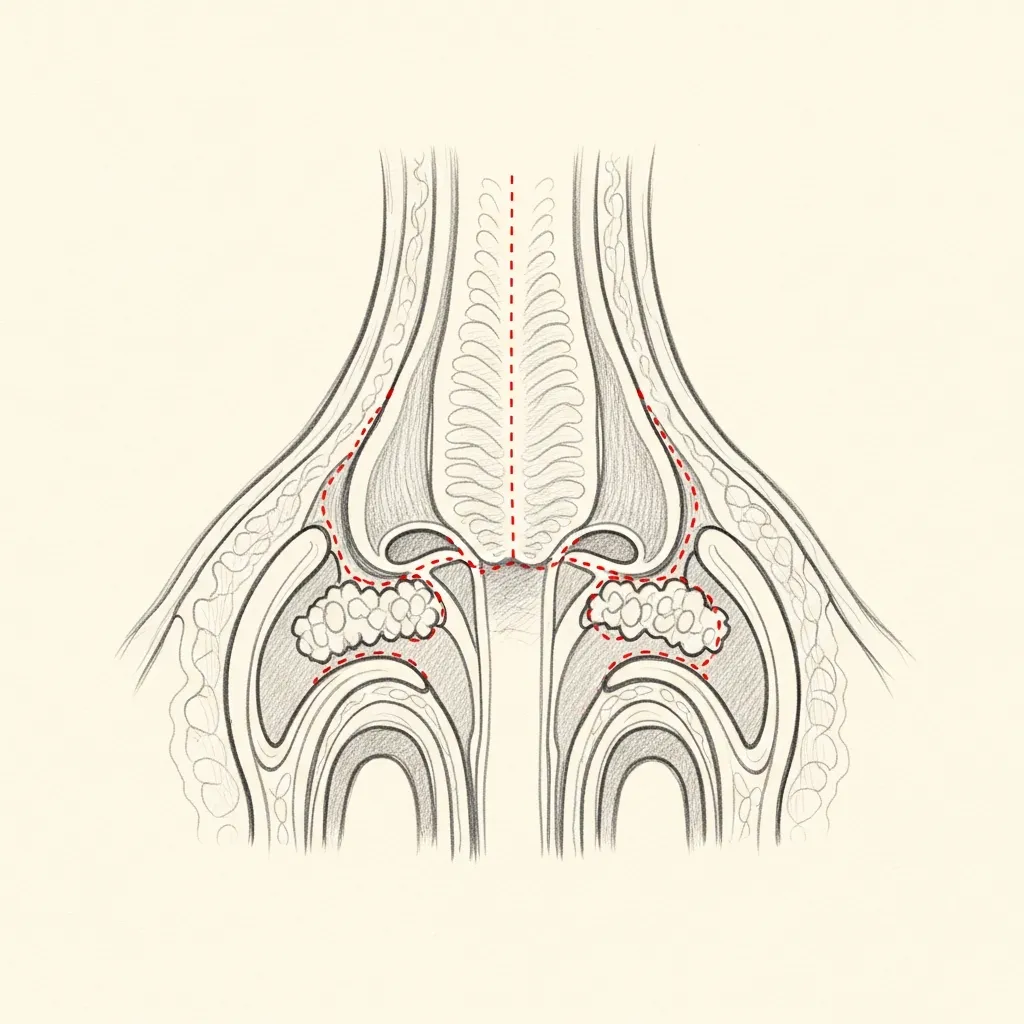
Polypectomy
Removal of polyp burden
Polyps are removed under endoscopic visualisation using powered instrumentation — preserving normal mucosa wherever possible.
The goal is to restore airway and drainage without removing healthy tissue. Aggressive stripping of mucosa is counter-productive and increases scarring.
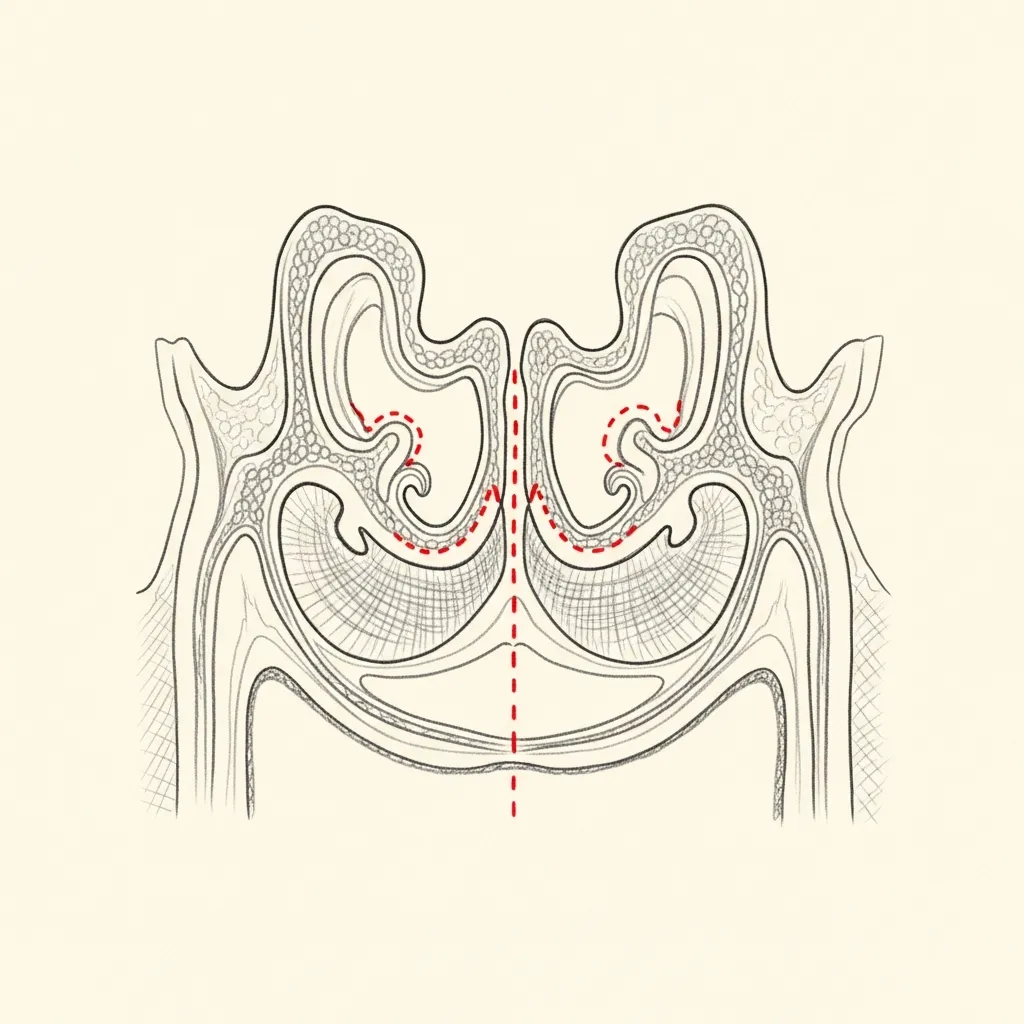
FESS
Opening sinus drainage pathways
Where polyps have obstructed sinus drainage, the natural outflow tracts are opened — most commonly the maxillary, ethmoid, and frontal sinuses.
Restoring drainage is what allows the medical plan after surgery to actually reach the sinus mucosa and control inflammation long-term.
Illustrative diagrams. The extent of surgery is decided case by case based on imaging and endoscopy.
Begin the conversation
A careful, honest evaluation is the right first step.
Cost, Financing & Insurance
Nasal Polyps Surgery Cost, Financing & Insurance in NYC
Nasal polyps surgery cost depends on the extent and location of the polyps, the degree of associated sinus disease, whether endoscopic sinus surgery or other nasal procedures are included, the type of anesthesia, and the surgical facility.
Because nasal polyps surgery treats a medical condition, it may be covered by insurance when it is medically necessary. Coverage often depends on symptoms, CT imaging, prior medical treatment, and the requirements of the patient’s insurance plan. Our office can help review benefits and guide patients through preauthorization when appropriate.
What May Affect Cost
- Extent and location of polyps
- Degree of sinus disease
- Whether endoscopic sinus surgery is included
- Type of anesthesia
- Prior medical treatment
- Insurance plan requirements
This information is educational and is not a guarantee of pricing, insurance coverage, reimbursement, financing approval, or surgical candidacy. A personalized estimate is provided after consultation. Insurance coverage depends on the patient’s plan, medical necessity, documentation, and carrier requirements. Financing terms are determined by third-party financing providers.
05 · In Dr. Mourad's Words
Educational videos.
Short educational films and patient perspectives from the Manhattan practice.
Dr. Mourad in Practice
An overview of the practice and philosophy.
Patient Perspective
A patient discusses her experience before, during, and after surgery.
Inside the Consultation
How Dr. Mourad evaluates anatomy, goals, and candidacy.
06 · Recovery
What healing actually looks like.
Stage 01
First 24 Hours
Initial recovery focuses on rest, hydration, and following all post-operative instructions exactly. Pain is managed with multi-modal non-narcotic protocols where appropriate.
Stage 02
Week 1
Swelling and bruising peak in the first few days and improve steadily through the first week. Most patients are presentable for casual social activity by the end of week two.
Stage 03
Weeks 2 – 4
Through weeks two to four the early result begins to settle. Light cardio resumes around three weeks; vigorous exertion and contact activities are deferred per the operative plan.
Stage 04
Months 1 – 6
The final refined result emerges progressively over the following months as residual swelling continues to resolve. Follow-up visits are scheduled across the first year.
Have a specific question?
Send a brief note describing your anatomy or concerns — the office will route it directly to Dr. Mourad for review.

Before You Arrive
Your consultation, prepared.
Bring photographs relevant to your concern, when available.
Bring records from any prior surgery, when available.
List current medications, supplements, and blood-thinning agents.
Note any prior anesthesia issues or chronic medical conditions.
Allow 60 minutes for the first consultation.
Bring questions; no decisions are made at the first visit.
Patient Perspectives
From patients of the practice.
I had lost my sense of smell completely for almost two years. A few weeks after surgery it began coming back, and that was a more meaningful change than I expected.
Dr. Mourad was honest that polyps can recur and that medical maintenance after surgery is part of the plan. That candor mattered to me.
Breathing through my nose at night has changed how I sleep. My partner says the snoring is gone, and I feel more rested.
Individual experiences. Results and recovery vary by patient. Testimonials shared with written consent.
At a Glance
Nasal polyps surgery fact snapshot.
- Treats
- Obstructing nasal polyps and the chronic rhinosinusitis with polyps that produces them, including loss of smell and persistent congestion.
- Does not treat
- The underlying inflammatory tendency — polyps can recur, so surgery is paired with ongoing medical therapy rather than replacing it.
- Evaluation
- Nasal endoscopy and CT imaging after optimized medical therapy with topical and sometimes systemic steroids.
- Related conditions
- Chronic sinusitis with polyps, aspirin-exacerbated respiratory disease, asthma, fungal sinusitis.
- Possible combined procedures
- Endoscopic sinus surgery of the involved sinuses, septoplasty, turbinate reduction.
- Recovery summary
- Most patients return to desk work within about a week; smell and congestion often improve as swelling settles, with saline rinses supporting healing.
- Insurance / functional distinction
- Polyp surgery is a functional, medically indicated procedure and may be submitted for insurance review — coverage is never guaranteed. This out-of-network practice provides documentation for reimbursement.
- When to seek evaluation
- When congestion, drainage, or loss of smell persists despite steroid sprays or rinses, or polyps are visible in the nostril.
Frequently Asked
Patient questions, honestly answered.
The decision integrates symptom severity, objective disease on endoscopy and CT, and response to medical therapy. If topical intranasal steroids and a monitored short oral steroid trial fail to control obstruction, recurrent infection, or smell loss, we consider endoscopic surgery to reestablish drainage. For patients with eosinophilic disease, aspirin‑exacerbated respiratory disease (AERD), or inadequate control after surgery, steroid‑sparing biologic agents may be appropriate (discussed with allergy/immunology). Final sequencing is individualized and agreed on in clinic with input from specialists.
Asthma commonly coexists with polyp disease and raises the index of suspicion for eosinophilic inflammation. We review pulmonary control, recent exacerbations, and inhaled steroid use before scheduling surgery and coordinate perioperative care with your pulmonologist. Postoperative plans often emphasize early topical nasal steroids, closer surveillance, and expedited allergy referral if control is suboptimal. In cases of AERD, timing of desensitization or biologic therapy is planned collaboratively.
Evaluation includes a focused history, in‑office nasal endoscopy, and a non‑contrasted sinus CT to map disease and ostial obstruction. Allergy testing or immunologic evaluation is ordered when clinically indicated, particularly for recurrent or refractory disease. Medication review addresses anticoagulants, aspirin, and systemic steroid exposure before scheduling. Imaging and endoscopy together determine the extent of required dissection and whether image guidance or staged procedures will be needed.
Options range from targeted endoscopic polypectomy to functional endoscopic sinus surgery (FESS) that selectively widens obstructed ostia. The operative strategy prioritizes mucosal preservation: remove polypoid tissue, restore natural drainage pathways, and avoid unnecessary mucosal stripping. Instruments commonly include angled endoscopes, microdebriders, suction, and careful bipolar or topical hemostatic measures. The exact extent of dissection is tailored to CT anatomy, prior surgery, and inflammatory phenotype.
Initial postoperative congestion and mild discomfort are typical for 24–72 hours; saline irrigations and topical steroids begin early to support healing. Many patients notice improved airflow within days as edema resolves, while measurable recovery of smell often continues over weeks to months and may improve up to 3–6 months in many cases. Scheduled clinic visits for endoscopic cleaning and surveillance occur in the first 1–4 weeks to manage crusting and assess mucosal recovery. Individual recovery varies with disease severity and prior operations.
Common risks include temporary bleeding, crusting, and infection, which are managed with topical care and antibiotics when appropriate. Less common but important risks include orbital injury, cerebrospinal fluid leak, and changes in vision; these are rare and managed promptly with specialist input if suspected. We use image guidance, careful dissection, and conservative hemostatic techniques to reduce risk. All patients receive preoperative counseling about these possibilities and written postoperative instructions.
Recurrence risk is driven by underlying inflammatory biology rather than the surgery itself; patients with eosinophilic disease or AERD have higher recurrence tendencies. Long‑term topical intranasal corticosteroids, regular saline irrigations, and close follow‑up with allergy or immunology reduce recurrence and preserve surgical benefit. For recurrent or medically refractory cases, biologic therapy or revision endoscopic surgery are considered after re‑evaluation. Surveillance intervals are individualized based on disease severity and response.
Revision procedures are more complex due to scar tissue and altered anatomic landmarks, which can lengthen operative time and necessitate angled endoscopes or image guidance. Preoperative CT imaging is essential to map prior dissections and locate retained disease or complications. Intraoperative strategy focuses on restoring drainage while conserving any remaining healthy mucosa. Patients are counseled about the possibility of staged surgery and more intensive postoperative surveillance.
Coverage depends on documented symptomatic disease and prior medical therapy; most insurers require evidence of failed appropriate medical management and objective findings on CT or endoscopy. Our administrative team assists with prior authorizations and with transmitting clinical records and imaging to payers. Preoperative clearance, scheduling at an accredited facility, and coordination with other specialists (allergy, pulmonology) are standard steps. Specific coverage questions are addressed during the scheduling process.
Clinical references
This page draws on published clinical practice guidelines and public-health references. These sources inform general patient education and do not replace an individual evaluation with Dr. Mourad.
- 01Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, et al. Clinical Practice Guideline (Update): Adult Sinusitis. Otolaryngology–Head and Neck Surgery. 2015;152(2_suppl):S1–S39. AAO-HNSF guideline
- 02U.S. National Library of Medicine (MedlinePlus Medical Encyclopedia). Nasal polyps. MedlinePlus
- 03U.S. National Library of Medicine (MedlinePlus). Sinusitis. MedlinePlus
The Most Important Step
Your expert consultation.
A careful evaluation by a double board-certified physician is the right first step. The conversation is unhurried, the diagnosis is honest, and the operative plan is built around what your anatomy can sustain and what you actually want.