Nose · Editorial Journal
Septoplasty vs. Rhinoplasty: Functional Surgery, Aesthetic Surgery, and When They Overlap
Two operations on the same anatomy with different goals — and how a dual-trained surgeon plans them as a single system when both are needed.
Two of the most frequent questions in a nasal consultation are also the two most commonly conflated. Septoplasty and rhinoplasty share anatomy and language, but they answer different questions — one functional, one aesthetic — and the choice between them, or the decision to perform them together, depends on a careful examination rather than a default recommendation.
Septoplasty: a functional operation
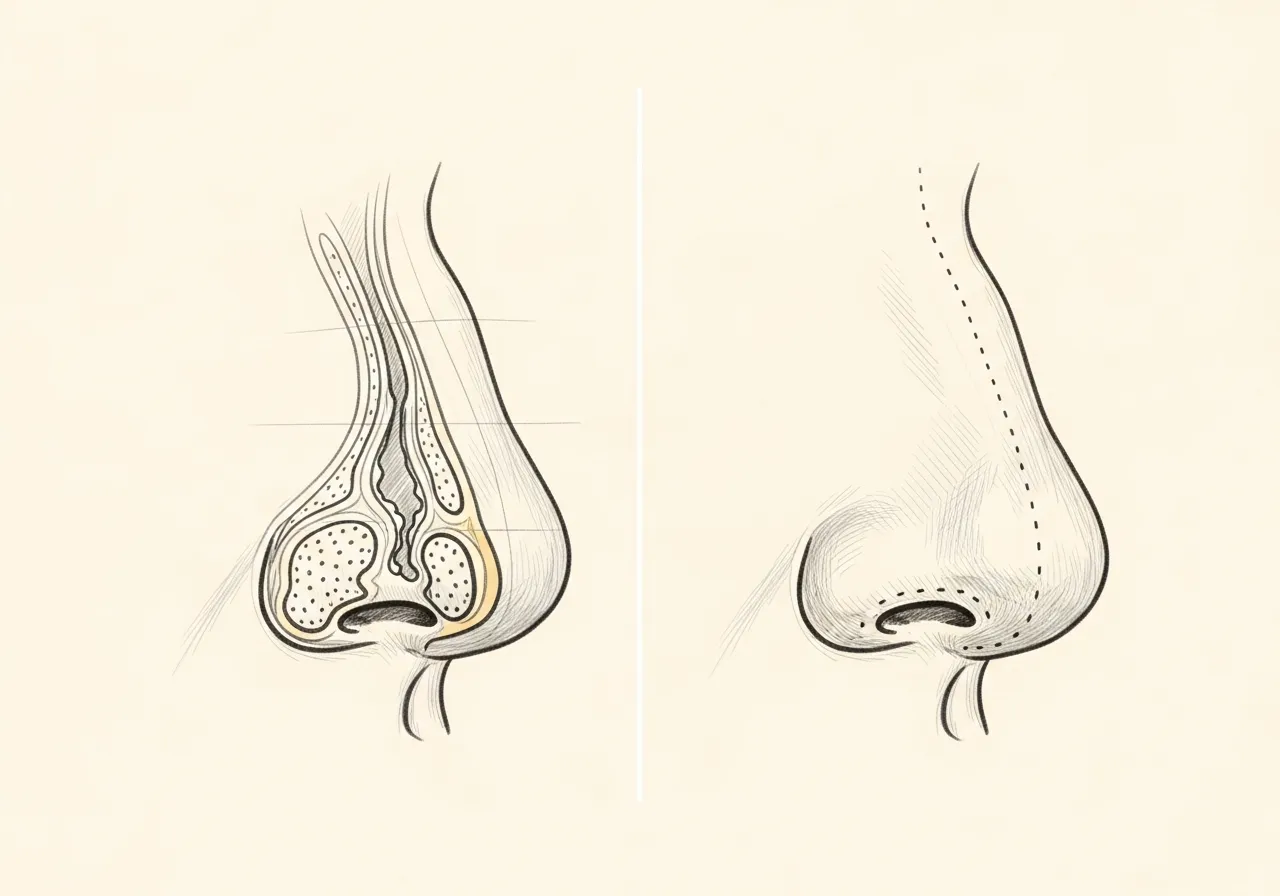
Septoplasty addresses the internal cartilaginous and bony partition that divides the nasal cavity into two passages. When the septum deviates from the midline — whether from genetics, prior injury, or progressive change — it can obstruct airflow, contribute to recurrent sinus infections, or interfere with sleep.
The operation is performed from inside the nose; there are no external incisions and no change to the external shape when septoplasty is done in isolation. The goal is straightforward — restore an open, symmetric internal airway. Because it is a functional procedure, septoplasty is frequently covered by insurance when a clear medical indication is documented.
Rhinoplasty: an operation of form and structure
Rhinoplasty addresses the external shape, proportion, and contour of the nose. It is a structural operation — the cartilaginous framework and bony pyramid are refined, supported, or rebuilt to alter how the nose looks in profile, on frontal view, and during animation.
Modern technique increasingly favors preservation of native structure where possible, rather than reduction for its own sake. Cartilage grafts and structural support play a major role; the operation is planned to age well over decades rather than to peak immediately after the splint comes off.
Where the two operations meet
A nose with both internal and external concerns is a common presentation. A patient who is bothered by the dorsal contour may also have functional obstruction from a deviated septum. A patient who breathes poorly may have associated external asymmetry from prior trauma.
When both are present, a septorhinoplasty performed in a single setting is often a reasonable approach. The structural support gained from the septum during septoplasty is also the cartilage frequently used for grafting during rhinoplasty; planning them together preserves anatomy that would otherwise be discarded.
"A rhinoplasty that compromises the airway has not been a success, no matter how the result photographs. The two operations are part of a single architectural problem."
How the consultation distinguishes the two
Diagnosis precedes any surgical recommendation. A complete examination includes external aesthetic evaluation, internal nasal endoscopy, and dynamic assessment of the nasal valves during breathing. Imaging is reviewed when indicated. Only after this is the conversation about technique — open, closed, preservation, or combined — appropriate.
Dr. Mourad's dual training in facial plastic surgery (ABFPRS) and otolaryngology (ABOto) means external aesthetics and internal function are evaluated in the same examination by the same surgeon, rather than handed between specialties. This is part of why the practice frequently sees patients whose prior surgery addressed one half of the problem.
Continue Reading